
Occurring at any time during pregnancy and up to a year after giving birth, perinatal mental illnesses include PPD (postpartum depression), sometimes called postnatal depression, and postpartum psychosis.
What is it?
Feeling tearful or irritable just after giving birth is so common it is dubbed the “baby blues,” but these feelings last for only a couple of weeks. What sets PPD apart from baby blues is the length of time it lasts. It is a longer-term moderate to severe depression that can develop in new mothers (and occasionally fathers) at any time in the year after birth. Symptoms include constant low mood or mood swings, low energy levels, difficulty bonding with the baby, and frightening thoughts. The individual may cry easily and profusely and feel acutely fatigued yet have sleep problems. Feelings of shame and inadequacy, worthlessness, and fear of failure as a parent are common. In severe cases, panic attacks, self-harm, and thoughts of suicide occur. However, most individuals make a full recovery. Untreated, PPD may last for many months or longer. PPD can develop suddenly or
slowly, and is usually caused by hormone and lifestyle changes and fatigue. It is not clear why some people develop PPD, but risk factors appear to include difficult childhood experiences, low self-esteem, a lack of support, and stressful living conditions.
How is it diagnosed?
To determine whether an individual has PPD, a doctor, midwife, or health professional assesses symptoms using an efficient and reliable screening questionnaire such as the Edinburgh Postnatal Depression Scale, which rates mood and activity levels over the previous seven days. Other assessment scales are used to assess mental well-being and functioning. Good clinical judgment is needed
when interpreting the results of these questionnaires as new parents are likely to be less active simply as a result of their new responsibilities.
POSTPARTUM PSYCHOSIS
An extremely serious condition, postpartum psychosis (also known as puerperal psychosis) affects 1–2 women per 1,000 births. It usually occurs in the first few weeks after delivery, but may begin up to six months after birth. Symptoms often develop rapidly and include confusion, high mood, racing thoughts, disorientation, paranoia, hallucinations, delusions, and sleep disturbance. The individual may also have obsessive thoughts about the baby, and attempt to self-harm or harm the baby. Immediate treatment is needed because of the
potentially life-threatening thoughts and behaviors associated with the disorder. Treatment comprises hospitalization (usually in a highly monitored mother-and-baby treatment unit), medication (antidepressants and antipsychotics), and psychotherapy.
TREATMENT
❯ Cognitive and behavioral therapies in a group, one-on-one, or as guided self-help; one-on-one counseling
❯ Lifestyle management, such as talking to partner, friends, and family; resting; regular exercise; and eating healthily and regularly.
❯ Antidepressants alone or with psychotherapy.
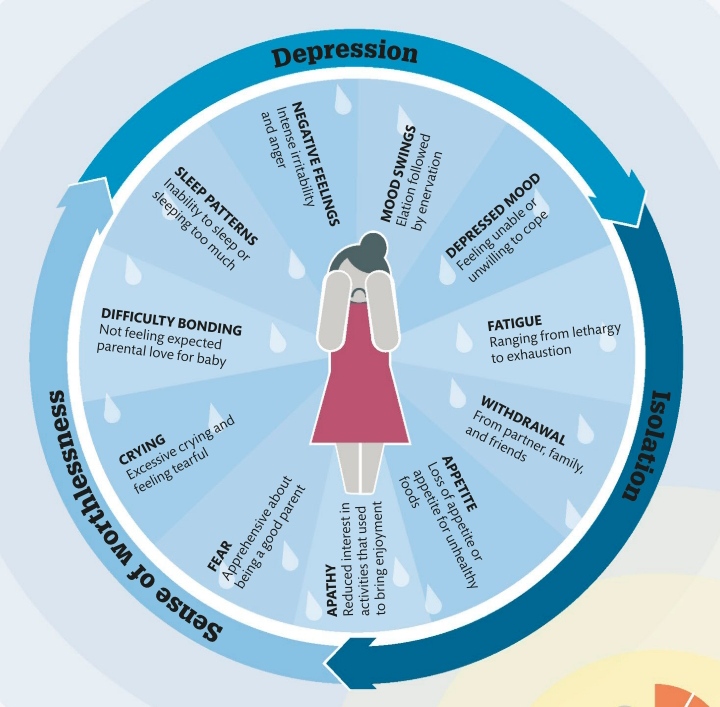
Range of symptoms
The symptoms of postpartum depression are similar to those of anxiety and general depression. Symptoms can make it difficult to complete day-to-day activities and routines, and can affect an individual’s relationship with their baby, partner, family, and friends.
85%
of new mothers experience the “baby blues”

Leave a comment