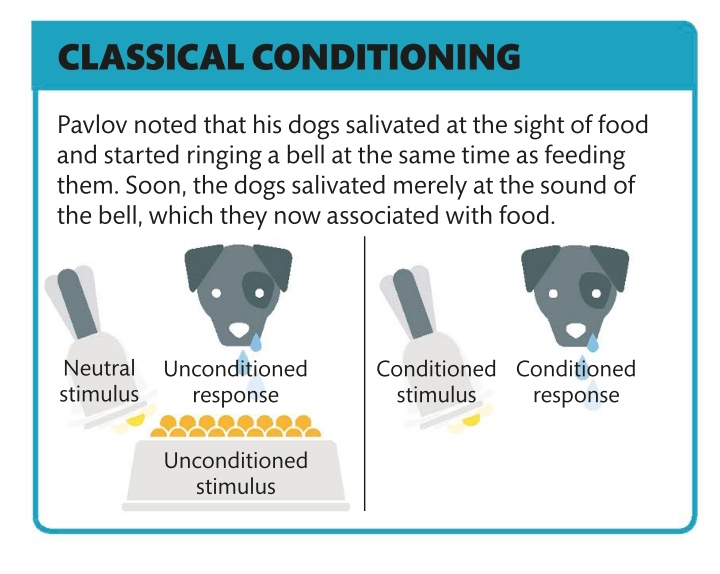
Instead of exploring the unconscious to shed light on the conscious mind, transactional analysis focuses on the three “ego states” of an individual’s personality
What is it?
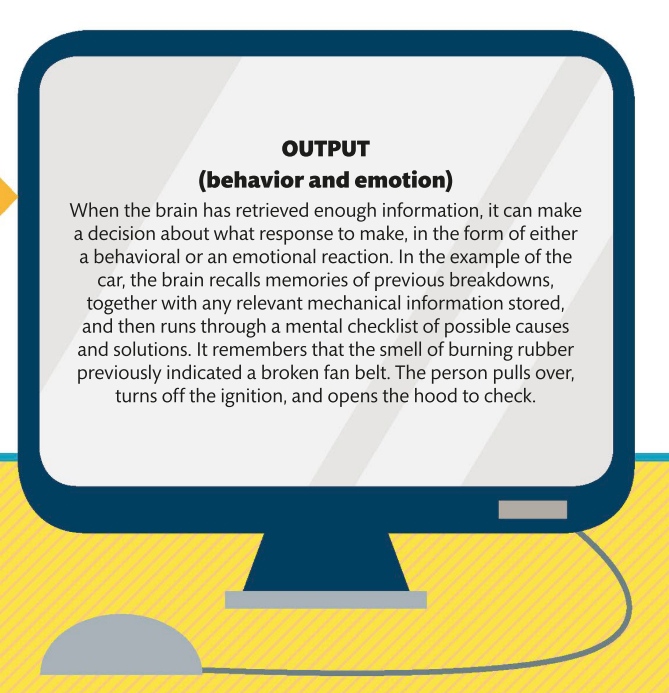
Rather than asking the client questions about themselves, the therapist observes and analyzes how they interact. Then they help the client develop a strategy for operating from the adult ego state, rather than copying how their caregiver treated them when they were young (the parent ego state) or acting out how that treatment made them feel and behave as a child (the child ego state). Conflict occurs when a person operates simultaneously from different states, for instance, one part of their personality giving orders from their parent state and another part reacting defensively from their child state. Transactional analysis helps the client to recognize these three states and guides them toward using their adult state in all interactions. It helps the client communicate as they wish to, unhindered by patterns formed in childhood. The adult state is based in the present, and evaluates data from the child and parent states to draw a logical, intelligent conclusion that directs behavior.
PARENT Can be controlling and critical or nurturing and supportive
ADULT Makes rational choices in response to the present time
Both of these therapies are offshoots of Freudian psychoanalysis. The therapist uses empathy to understand the client’s unique perspective of life and create patterns of behavior that improve relationships.
What are they?
IN OBJECT RELATIONS, the therapist helps the client relinquish relationships from childhood and replace them with models of behavior appropriate to their adult life.
Both self psychology and object relations focus on experiences in a client’s early life as a way to understand and improve their adult relationships. The premise of self psychology is that children deprived of empathy and support in their early years cannot develop self-sufficiency and self-love as adults. The therapist fulfills the client’s urge to look to others to meet their needs, giving them the self-worth and self-awareness to carry into their own relationships. In object relations—the name for childhood relationships that the adult is repeating inappropriately—the aim is to use the empathy with the therapist as a platform for analyzing past interactions and emotions and applying new positive models of behavior.
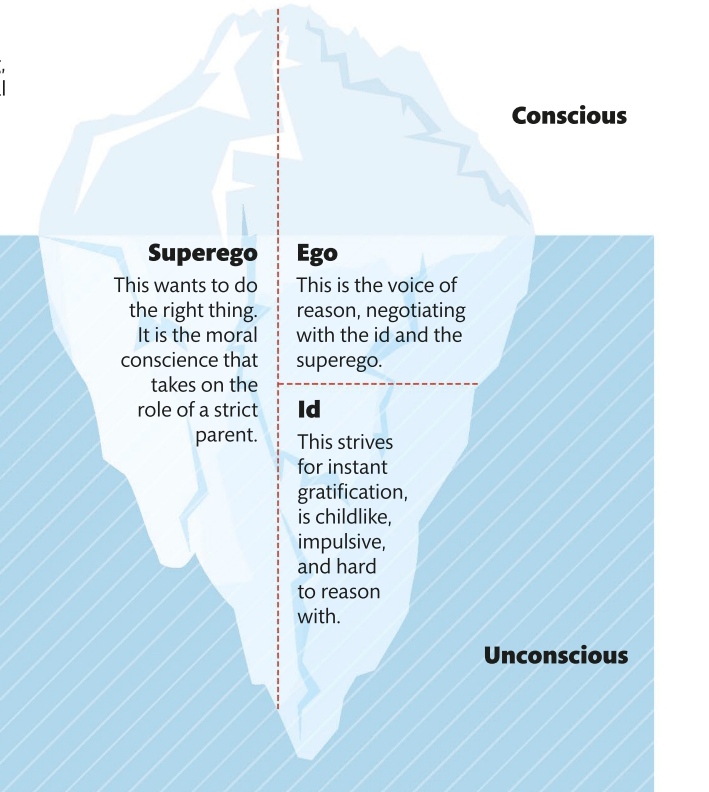
Carl Jung expanded Freud’s ideas—he thought the unconscious mind went far deeper than the merely personal and was at the core of behavior patterns.
What is it?
Like his colleague Sigmund Freud, Jung considered that psychological distress occurs when the conscious and unconscious parts of the mind are unbalanced. But Jung thought that personal memories were part of a much larger whole. Jung noticed that the same myths and symbols occur across the world, whatever the culture. He thought these must be the result of shared experience and knowledge of the human species, remembered by everyone as what he called the collective unconscious. These memories, in the deepest layer of the unconscious mind, take the form of archetypes—instantly recognizable symbols that shape behavioral patterns. The conscious ego is the public image that a person presents to the world. Its archetype is the persona, identifiable as a person being on their best behavior. The darker aspects of the mind that most people hide Jung called the shadow. Further archetypes are the anima (female traits in men) and the animus (male traits in women), which often clash with the conscious ego and the shadow. To find the true self, all the layers of a person’s personality need to work in harmony. Whereas psychoanalysis delves into the top layer of the client’s unconscious, Jungian therapists explore all the layers. Their role is to help the client use the archetypes to understand and change their own behavior. Jungian therapists use techniques such as dream analysis and word association to reveal where the inner archetypes collide with outer-world experiences. This process of analysis enables the client to understand which layers of their mind are in conflict, and then make positive changes to restore the balance. Like psychoanalysis, this therapy is a fascinating journey into the mind and can take years.
NEED TO KNOW
❯ Word association The client says whatever comes into their mind when the therapist presents them with a word.
❯ Extrovert Someone whose attention is directed toward the outside world and other people; outgoing, responsive, active (even reckless), decisive.
❯ Introvert Someone whose attention is directed inward to their own thoughts and feelings; shy, contemplative, reserved, self-absorbed, indecisive.
The purposes of psychoanalysis and psychodynamic therapy as specific methods are similar—to integrate the unconscious and conscious mind—but the depths of the processes differ.
What is it?
The founder of psychoanalysis, Sigmund Freud, developed his “talking therapy” after working in Paris with Jean-Martin Charcot, a neurologist who discovered that his patients’ symptoms lessened after they talked about past traumas. In the early 1900s, Freud established techniques such as free association, dream analysis, and resistance analysis, still widely used today. Silences in therapy are often as meaningful as what is said. All psychoanalysis assumes that psychological problems stem from the unconscious; that unresolved issues or repressed trauma hidden in the unconscious mind cause symptoms such as anxiety and depression; and that treatment can raise these conflicts to the surface so the client can resolve them.Psychoanalysis often takes years, deconstructing and rebuilding the client’s entire belief system. It benefits those who are robust of mind, with an outwardly successful life, but are aware of long-term worries or torments, such as an inability to stay in a relationship. Psychodynamic therapy is less intense and focuses on present-day problems, such as a phobia or anxiety.
INTERPRETATION The therapist stays relatively quiet, reading between the lines of what the client says to help them overcome subconscious limitations.
THE THERAPIST The analyst listens but does not judge so that the client need not fear saying something shocking, illogical, or silly.
An umbrella term for all analytic therapies, psychodynamic therapy is also a method in itself. Analytic therapies follow the root aim of Sigmund Freud—to bring the unconscious mind into consciousness.
What are they?
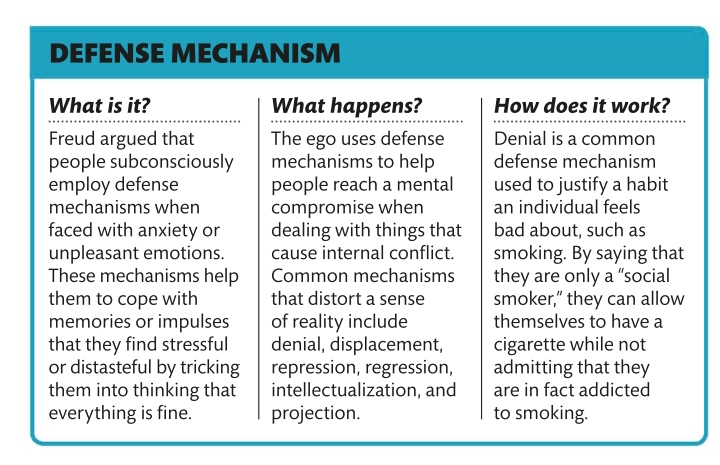
The principle behind the psychodynamic approach is that the unconscious mind harbors feelings and memories, particularly from childhood, that shape thought patterns and behavior in adulthood. The therapist helps the client to talk about these often unwanted feelings and so draw them into the conscious mind. Burying unpleasant memories results in anxiety, depression, and phobias, and bringing them into the light of day gives the client the tools to resolve their psychological problems as an adult. Acknowledging buried memories helps the client to identify, confront, and ultimately change the defense mechanisms they have developed to avoid experiencing painful realities or facing unpleasant facts and unwanted thoughts. These (usually unconscious) mental strategies include denial (refusal to accept reality), repression (burying an unwanted thought or feeling),compartmentalization (mentally separating conflicting emotions or beliefs), reaction formation (acting contrarily to how the person feels), and rationalization (self-justifying an unacceptable behavior). In all psychodynamic therapies, the therapist listens to the client talking about their conscious problems while looking for patterns, behaviors, and emotions that hint at their subconscious feelings. The goal is to enable the client to deal positively with inner conflicts.
The session
All forms of psychodynamic therapy take place in a familiar, safe, respectful, nonjudgmental environment. Sessions are usually one-on-one and last 50–60 minutes.
DREAM ANALYSIS A means of accessing the unconscious, analyzing dreams can reveal hidden emotions, motivations, and associations.
RESISTANCE ANALYSIS Showing the client what, how, and why they are resisting in thoughts, ideas, or emotions can explain defense mechanisms.
FREUDIAN SLIP The client reveals what is really on their mind (their unconscious thought) by saying something they did not intend to.
THE CLIENT In traditional Freudian analysis, the client lies on a couch and cannot see the therapist. In more interactive forms, the client can see the therapist.
FREE ASSOCIATION The client talks spontaneously about whatever comes to mind, without editing what they say or attempting to give a linear structure. True thoughts and feelings emerge.
TRANSFERENCE The client’s unconscious conflicts surface in their relationship with the therapist. They redirect emotions and feelings, often from childhood, from themselves to the therapist.
Psychotherapies use a range of strategies to help people modify the thoughts, actions, and emotions that are harmful to their physical or mental health, and also to promote improved self-awareness.
Therapeutic action
Psychotherapies are often referred to as “talking therapies” because communication with a therapist is the key agent for change. The aim is to manage adversity; maximize potential; clarify thought; provide support, encouragement, and accountability; and cultivate peace of mind and depth of consciousness. Therapy seeks to improve a client’s understanding of themselves, others, and their relational dynamics. It may also be used to define personal goals and organize behavior into achievable systems.Psychotherapy can uncover old wounds and help a client understand how past negative experiences currently affect them in unhealthy ways. It can also help them change the ways they react to external stimuli, and how they internally process and interpret experiences, allowing them to move beyond current states of thought and behavior. Therapy can empower a client to explore their psyche and spiritual self and to achieve more satisfaction in their lives. It is designed to increase self-acceptance and self-confidence, and to diminish unhelpful negative or critical thinking.
Types of therapy
Therapeutic approaches and methods are as diverse and creative as the mind itself, and psychological progress can be achieved in many ways. The main types of therapy are categorized according to the philosophy on which they are based. Methods of delivery vary and might comprise individual sessions, group therapy, or online guidance and task completion.
PSYCHOANALYTICAL AND PSYCHODYNAMIC
These approaches are based on the concept that unconscious beliefs underlie maladaptive thoughts and behaviors. Gaining an insight into these beliefs can explain and relieve problems. The therapist and client also work to develop healthier ways of dealing with these previously repressed feelings, and to foster the client’s inner resources and capability to manage their troubles.
COGNITIVE AND BEHAVIORAL
These therapies stem from the belief that it is not the things that happen to a person that upset them, but it is the way they think about the things that happen to them, and the meaning that they assign to their experience, that upsets them. Cognitive and behavioral therapies show people that they hold the power to change the way they think about things, and the way they react and behave as a result of these thoughts.
HUMANISTIC
This approach prioritizes listening over observing. To this end, therapists use open-ended questions and qualitative tools to study personality and encourage the client to explore their own thoughts, emotions, and feelings. The therapist sees the client as inherently capable of and responsible for achieving personal growth, and not as a set of flawed unconscious drives.
SYSTEMIC
The “systems” approach enables people to work out issues arising from the interplay of relationships. Therapists can gain deeper understanding of problems by working with everyone in a system (family or group), hearing differing points of view, and watching people interact. This allows people to explore their identity as part of a larger group, and also has the advantage of strengthening their community network—useful for issues that worsen with isolation, such as addiction.
ROLE OF MEDICINE The brain and behavior exert a continual reciprocal influence on one another. Medication can alter brain chemistry to improve mood, concentration, memory, and motivation; increase energy; and decrease anxiety. This improved functioning can alleviate the symptoms of mental illness and enable positive behavioral change.
GROUP THERAPIES
12-step program The 12-step model is a group therapy approach specifically used to tackle addictions (such as to drugs, alcohol, or sex), and compulsive behaviors like eating disorders. An essential part of overcoming addictions or compulsions is support from and connection to a community. Group therapy reduces isolation and associated shame, shows people that they are not alone in their struggle, and provides a network for support and accountability.
SHARING EXPERIENCES in a group allows people to give and receive support and feedback, and to pool strategies for change
Self-help groups These support groups focus on self-disclosure. Whereas some groups have a professional lead, others are peer-led. Shared experience is valued over professional knowledge.
28% of people in the UK have consulted a psychotherapist
Scientific research increasingly links our mental health with physical health, and psychologists in this field have developed tools for assessing, and improving, our mind‑body connection.
Making the connection
Health psychologists explore how a person’s state of mind (someone, for example, suffering from the day-to-day experience of stress) affects their body, and they find ways to improve a person’s physical health by helping them change the way they think. This may involve changing their lifestyle, social network, and attitude and perceptions. Health psychologists work in a variety of roles—in the community to help vulnerable and sick people, advising public authorities on health policy, and in hospitals.When assessing an individual, the psychologist looks at all the factors that may contribute to an illness or a problem, and devises a strategy for change. This might include identifying behaviors that damage a person’s health, such as smoking or poor diet; encouraging positive behavior such as exercise, a healthy diet, oral hygiene, health checks, and self-examination; improving sleep practices; and scheduling preventive medical screenings. Health psychologists may also promote cognitive behavior changes that give the person more control over their life.
Managing health conditions
Health psychologists can help when people are diagnosed with conditions that require hospitalization or prolonged treatment, such as cancer, or alcohol or drug addiction. The psychologist will assess what can be changed to help improve the person’s ability to cope mentally with physical pain or discomfort and the potentially life-changing impact of their condition. A diverse range of strategies are also employed to aid rehabilitation. On the psychological front, health psychologists work to build and maintain a patient’s self-esteem and motivation, training them to think more positively. Rallying the support of friends, family, and other health professionals is part of this process. On the physical side, they may implement alternative therapies, such as yoga and acupuncture, to enhance a patient’s well-being, help control cravings, or overcome depression. They may also recommend regular exercise, a nutrition program, or vitamin therapy.
Biopsychosocial model
Health psychologists use this model to assess three different forces meshing like a honeycomb in a person’s life: biological (the impact of physical traits); psychological (thought patterns and attitudes); and social (the influence of life events and other people). Psychologists recognize that these three forces can have either a positive effect or a negative effect on health and well-being.
FORCES FOR HEALTH
BIOLOGICAL A healthy diet, exercise, a life free from addictions, time to relax, and no genetic predisposition to illness.
PSYCHOLOGICAL Stress management, positive thoughts, resilience, mental discipline, and giving and receiving love.
SOCIAL The support of social groups such as friends, family, and religious or other communities, along with access to medical care and health education.
FORCES AGAINST HEALTH
PSYCHOLOGICAL Stress; anxiety; poor coping skills; negative thoughts; and pessimistic, suspicious, or overly aggressive personality.
BIOLOGICAL Poor diet, a genetic predisposition to illness, smoking, pollution, and excessive alcohol or drug
SOCIAL Loneliness; poverty; exploitation; and exposure to violence, abuse, or relationship trauma.
RATING MENTAL HEALTH
When a formal assessment is needed, psychologists use a questionnaire to rate or measure an individual’s state of mind, differentiating between psychological health and emotional well-being.
Psychological health questions
❯ Mood Is your mood generally positive?
❯ Positive relationships Do you have friends or positive emotional ties?
❯ Cognitive function Can you properly think and process information?
Emotional well-being questions
❯ Anxiety Do you suffer from anxiety?
❯ Depression Are you depressed?
❯ Control Do you feel you have lost control or cannot control your feelings?
HOW STRESS AFFECTS THE BODY
Stress is nature’s way of alerting people to danger, putting their bodies into primitive “fight-or-flight” mode . The brain produces a cocktail of chemicals in response to stress, triggering changes throughout the body.
NERVOUS SYSTEM Headaches, irritability, nervousness, heightened sensitivity
CARDIOVASCULAR SYSTEM Fast heartbeat, raised blood pressure
RESPIRATORY SYSTEM Rapid, shallow breathing as muscles tense
GASTROINTESTINAL SYSTEM Diarrhea, nausea, constipation, stomach pain, heartburn
MUSCULOSKELETAL SYSTEM Muscle aches and pains, especially in neck, shoulders, and back
REPRODUCTIVE SYSTEM In women: irregular periods, reduced libido; in men: impotence
Psychologists working in the area of health aim to improve the mental and associated physical health of individuals, specific groups, and the wider population. This involves devising and delivering therapies to prevent and treat mental disorders, and to promote general wellness. They also play a role in evaluating how therapies improve health and which are the most effective. This influences the way psychological treatments are delivered at both the individual and public level.
Roles of a psychologist
Whether working independently, as part of an interdisciplinary health-care team, or in a research institution, psychologists are concerned with improving mental health and general well-being. Their different roles reflect the varied ways of achieving this goal for individuals or groups.
Health psychologist
What do they specialize in? These specialists look at how people deal with illness and the psychological factors that influence their health. They may research and deliver strategies to improve health and prevent disease, for example, promoting weight loss or stopping smoking, or may help individuals manage specific illnesses such as cancer or diabetes.
Who would benefit from their help?
❯ Chronically ill patients needing help adjusting to a serious illness or managing pain.
❯ Population groups needing lifestyle advice to prevent disease.
❯ Health-care providers wanting to know how to improve their services.
❯ Patient groups such as diabetics, who need advice to help them manage their condition.
Where would you find them?
Hospitals, community health settings, public health departments, local authorities, research institutions.
Qualifications
Doctoral level of education, followed by practical training, and continuing professional development.
Clinical psychologist
What do they specialize in?
These psychologists help people to deal with mental and physical health issues such as anxiety, addiction, depression, and relationship issues. After clinically assessing an individual using tests, discussion, or observation, they will provide appropriate therapy.
Who would benefit from their help?
❯ People with anxiety or depression in need of individual or group therapy sessions.
❯ Children with learning difficulties or behavior problems.
❯ Substance abusers who need help to tackle their addiction.
❯ PTSD sufferers in need of therapy to overcome past traumatic events and experiences.
Where would you find them?
Hospitals, community mental health teams, health centers, social services, schools, private practice.
Qualifications
Doctorate in clinical psychology.
Counseling psychologist
What do they specialize in?
These specialists help people facing difficult life issues, such as bereavement or domestic violence, as well as those with mental health disorders. They build a strong client relationship to effect change, and may also undergo therapy to inform their practice.
❯ Children experiencing social, emotional, or behavioral problems, or who have suffered any type of abuse.
❯ Sufferers of stress who can be helped to address underlying problems.
❯ Bereaved individuals needing emotional support and guidance.
Where would you find them?
Hospitals, community mental health teams, health centers, social services, industry, prisons, schools.
Qualifications
Doctoral level of education, followed by practical training, and continuing professional development.
PSYCHOEDUCATION
Increasing people’s awareness of living with mental health issues has become a key part of the therapeutic process. Whether delivered individually, in groups, or electronically via the Internet, psychoeducation helps those with mental disorders better understand their condition and the treatments, and also helps their families, friends, and caregivers provide more effective support. Having detailed information allows people to take better control of their lives and take positive steps to deal with their symptoms. It also improves a person’s compliance with treatment and can play a role in reducing the stigma often associated with mental health disorders.
WHO CAN PROVIDE TREATMENT?
Many mental health specialists can deliver psychological assessments, therapies, and counseling, but only some can prescribe medications to treat disorders.
Psychologists These professionals perform psychological assessments and deliver a range of talking or behavioral therapies, depending on the needs of the individual or group.
Psychiatrists These are medical doctors who specialize in the treatment of mental disorders. They are licensed to prescribe psychiatric drugs as part of a patient’s treatment.
General medical professionals Doctors (GPs and hospital consultants) and advanced psychiatric nurses can prescribe drugs or other therapies.
Other mental health specialists Social workers, psychiatric nurses, and counselors may deliver therapy alone or as part of a mental health team.
More than 75% of GP appointments in the US are attributed to issues related to stress and anxiety
These are disorders in which individuals display persistent and consistent unhealthy patterns of thinking, behavior, and social functioning.
What are they?
Individuals with PD have difficulty not only understanding themselves, but also relating to other people. PD is different from other mental illnesses due to its enduring nature and the fact that it cannot be compared to a physical illness. The individual’s behavior varies noticeably from the norm in society, but they may manage their own life without medical help in a way that someone with an extreme condition such as schizophrenia cannot. PD often goes hand in hand with substance abuse , depression , and anxiety. The precise causes of personality disorders are not known, but risk factors appear to include a family history of a personality or other mental disorder; an abusive, unstable, or chaotic early life; or a diagnosis of severe aggression and disobedience in childhood. Variations in brain chemistry and structure may also play a role. There are 10 defined PDs and they are considered to fit into three clusters based on broad similarities within each group. A doctor does not usually attempt a diagnosis of PD until early adulthood. For a diagnosis to be made, the symptoms must cause day-to-day problems with functioning and subjective distress, and the person must display some symptoms of at least one of the types.
Cluster A: odd/eccentric
A person with a Cluster A personality disorder shows patterns of behavior that most onlookers would regard as odd and eccentric, has difficulty relating to other people, and fears social situations. The individual may not believe that they have a problem. This group includes three personality disorders: paranoid, schizoid, and schizotypal.
Paranoid PD
person is extremely distrustful and suspicious.
❯ They think other people are lying to them, trying to manipulate them, or passing on shared confidences.
❯ They find hidden meanings in innocent remarks.
❯ They have problems maintaining close relationships, often believing that a spouse or partner is unfaithful despite a lack of evidence, for instance.
❯ Their suspiciousness and hostility may be expressed in overt argumentativeness; recurrent complaining; or quiet, hostile aloofness.
❯ The person’s hypervigilance for potential threats makes them appear guarded, secretive, devious, and lacking in tender feelings.
Schizoid PD
❯ The person appears cold, detached, and indifferent to other people.
❯ They prefer to take part in activities alone.
❯ They have little desire to form close relationships of any kind, including sexual ones.
❯ They have a limited range of social expression.
❯ They cannot pick up social cues or respond to criticism or praise.
❯ They have limited ability to experience pleasure or joy.
❯ They are more likely to be male than female.
❯ They may have a relative with schizophrenia
Schizotypal PD
❯ The person becomes very anxious and introverted in social situations, even familiar ones.
❯ They make inappropriate responses to social cues.
❯ They have delusional thoughts, attaching undue and misguided significance to everyday events. For example, they may be convinced that a newspaper headline contains secret messages for them.
❯ They may believe in special powers such as telepathy or their own magical ability to influence another person’s emotions and actions.
❯ They may have unusual ways of speaking, such as making long, rambling, vague statements or changing the subject partway through.
PEOPLE WITH PD often do not see themselves as having a problem so seeking treatment is rare.
TREATMENT
❯ Paranoid PD Schema-focused cognitive therapy to enable links between problems, for example, emotions from childhood memories and current life patterns; also uses cognitive techniques to develop new appraisals. However, high dropout rates from treatment occur, even if sought, due to difficulty in building rapport and trust between therapist and patient.
❯ Schizoid PD Cognitive behavioral therapy or lifestyle support to reduce anxiety, depression, angry outbursts, and substance abuse; social skills training; medication prescribed for low mood or psychotic episodes. However, treatment is rarely sought.
❯ Schizotypal PD Long-term psychotherapy to build a trusting relationship and cognitive behavioral therapy to help with identification and reevaluation of irrational thoughts; medication prescribed for low mood or psychotic episodes.
Cluster B: dramatic/emotional/erratic
A person suffering from a Cluster B personality disorder struggles to regulate their feelings. They are usually overly emotional and unpredictable and display behavior patterns that others see as dramatic, erratic, threatening, and even disturbing. This creates a vicious cycle, as people are uncomfortable near them, so social and personal relationships are difficult to achieve and maintain, which in turn intensifies the initial symptoms.
PSYCHOPATHY
Sometimes considered a subset of antisocial personality disorder (below), psychopathy is one of the hardest disorders to diagnose and is largely resistant to treatment. Psychopathy presents as a specific set of personality traits and behaviors. Mental health professionals can use Robert Hare’s Psychopathy Checklist-Revised (PCL-R) to diagnose the disorder by scoring an individual on 20 listed traits with a value of 0, 1, or 2. A score of 30 and above in the US, or 25 and above in the UK, results in a diagnosis of psychopathy. Interpersonal traits include grandiosity, deceit, and arrogance; emotion-based traits, lack of guilt and empathy; and impulsive traits, sexual promiscuity as well as criminal behaviors such as stealing. Individuals lack inhibition and do not learn from experience. They can seem charming at first, but their inability to feel guilt, empathy, or love, along with the presence of casual, reckless attachments and behavior, quickly becomes evident. Many traits—especially the ability to make clear, emotion-free decisions—can be found in successful individuals, particularly in business and sports. Most psychopaths are men, and the disorder is unrelated to the society or culture they come from.
Antisocial PD
❯ The person manipulates, exploits, or violates the rights of others.
❯ They see other people as vulnerable and may intimidate or bully them without remorse. They can be aggressive, even violent.
❯ Their behavior is often criminal; they lie and steal, and use aliases to deceive people.
❯ They disregard their own and others’ safety.
❯ They are consistently irresponsible and impulsive and have no concern for the consequences of their actions.
❯ They blame other people for problems they encounter.
❯ The disorder becomes evident in late teens and often dissipate by middle age.
Borderline pd
❯ The person has a fragile self-image.
❯ They are emotionally unstable (also called affect dysregulation), with severe mood swings and frequent, intense displays of anger.
❯ They have intense but unstable relationships with other people. ❯ They fear being alone or abandoned and have long-term feelings of emptiness and loneliness, leading to irritability, anxiety, and depression. ❯ They have disturbed patterns of thinking or perception (called cognitive or perceptual distortions).
❯ They act impulsively, with a tendency to self-harm and suicidal thoughts
Histrionic PD
❯ The person is self-centered and regularly seeks attention.
❯ They dress or behave inappropriately, and draw attention to themselves through physical appearance.
❯ Their emotional states rapidly shift, which makes them appear shallow. ❯ They are excessively dramatic, with exaggerated displays of emotion. ❯ They constantly seek reassurance or approval.
❯ They are suggestible (easily influenced).
❯ They believe that their relationships are more intimate than they are.
❯ They may function at a high level in social and work environments.
Narcissistic PD
❯ The person has an exaggerated sense of selfimportance, expects to be recognized as superior, and exaggerates their talents.❯ They are preoccupied with fantasies about success, power, brilliance, beauty, or the perfect partner. ❯ They believe they can associate only with people of equal importance. ❯ They expect special favors and unquestioning compliance from others and take advantage of them to get what they want. ❯ They are unwilling and unable to recognize anyone else’s needs and feelings.
❯ They believe they are envied.
TREATMENT
❯ Antisocial PD Cognitive behavioral therapy ; however, person may seek help only when ordered to do so by court because of their criminal behavior.
❯ Borderline PD Dialectical behavior and mentalizationbased therapies combining psychodynamic , cognitive behavioral , systemic , and ecological approaches, and art therapy . Group psychotherapy if symptoms are mild; coordinated care program for moderate-to-severe symptoms.
❯ Histrionic PD Supportive and solution-focused psychotherapy to enable emotion regulation; however, treatment is difficult as individual often exaggerates ability to function.
❯ Narcissistic PD Psychotherapy to help the person understand the cause of their emotions and regulate them.
Cluster C: anxious/fearful
This group of personality disorders is characterized by worried, fearful thinking or behavior. A person with one of these disorders struggles with persistent and overwhelming feelings of fear and anxiety and may show patterns of behavior that most people would regard as antisocial and withdrawn. Cluster C includes dependent, avoidant, and OC (obsessive compulsive) PDs. A psychiatric assessment is needed to differentiate between dependent (below) and borderline PD , because the two share some symptoms.
Dependent PD
❯ The person fears being on their own and having to fend for themselves. ❯ They constantly try to please and avoid disagreeing with people, because they are afraid of disapproval. ❯ They are oversensitive to criticism and pessimistic.
❯ They lack self-confidence, suffer from self-doubt, belittle their abilities and assets, and may describe themselves as “stupid.” ❯ They display needy, passive, submissive, and clinging behavior, and may tolerate abuse. ❯ If a close relationship fails, they urgently seek another one.
❯ They are often unable to start tasks for fear of failure.
Avoidant PD
❯ The person fears criticism, disapproval, or rejection so strongly that they find it difficult to make connections with people. ❯ They are extremely cautious in creating friendships.
❯ They are reluctant to share personal information or feelings, which can make it difficult to maintain the relationships they do have. ❯ They avoid any work activities that involve interpersonal contact. ❯ They stay away from social situations because they strongly believe they are inadequate and inferior.
❯ They worry constantly about being “found out” and others rejecting, ridiculing, or shaming them.
Obsessive compulsive PD
❯ The person is preoccupied with orderliness, perfectionism, and mental and interpersonal control.
❯ They are rigid and stubborn in pursuit of their principles. ❯ They are so devoted to work that they neglect friends and other activities, so they do not form or maintain meaningful social relationships. ❯ They are overconscientious and scrupulous and may miss work deadlines because they persistently aim for perfection.
❯ They are inflexible on matters of morality or ethics.
❯ They are unable to discard worn-out or worthless objects even when they have no sentimental value.
10% the estimated percentage of the global population affected by some form of personality disorder
Tics are sudden, painless, nonrhythmic behaviors that are either motor (related to movement) or vocal. A disorder may be diagnosed when tics occur repeatedly and are apparently unconnected to the environment or situation.
What are they?
Tics—small, uncontrollable movements or sounds— are not usually serious and normally improve over time. However, if they persist they can be frustrating and interfere with everyday activities—especially if the person has more than one tic. Changes in the parts of the brain that control movement are thought to cause tics. There is probably a genetic predisposition, too. Taking drugs such as amphetamines or cocaine can trigger tics, as can medical conditions, including cerebral palsy and Huntington’s disease, or psychological disorders such as ADHD and OCD . Tics are more common in children, but they can begin in adulthood. Statistics vary regarding the prevalence, with 0.3–3.8 percent of children described as having severe tics. Treatment may not be needed if a tic is mild; lifestyle management, such as avoiding stress or tiredness, is often all that is required.
Simple and complex tics
Tics take many forms. Some affect body movement and others are verbal. They may be simple or complex. A simple tic affects a small number of muscle groups, for example, blinking or clearing the throat. A complex tic involves coordinated patterns of several muscle groups, such as blinking in combination with a shoulder shrug, facial grimace, and spontaneous shouting.
This is a condition characterized by multiple tics, named after George de la Tourette, who first described it in 1884. For a condition to be classified as Tourette’s syndrome, the tics must last for at least a year and at least one must be vocal. Most individuals have a combination of motor and vocal tics, which can be both simple and complex. The syndrome often runs in families. Tourette’s syndrome is thought to be linked to TWISTING THE BODY problems with a part of the brain called the basal ganglia, or possibly to a childhood throat infection caused by a streptococcal bacteria. The first stage of diagnosis is to check other possible causes of the symptoms such as allergies or poor eyesight. A neurologist or psychiatrist then rules out conditions such as ASD before referring the person for psychotherapy. In a third of cases, the tics reduce, become less troublesome, or disappear over a 10-year period.
ADVANCE WARNINGS
Most people have an unusual or uncomfortable feeling before the tic occurs. Individuals often describe this as a rising tension that only the tic itself can release. Some people can suppress their tics for a short period, until the urge to do it becomes too strong, which may result in a more severe tic.
WARNING URGE
Burning sensation behind eyes
Tension in a particular muscle
Dry throat
Itching
NEED TO RELEASE TENSION
TIC
Blinking
Twitching individual muscle
Grunting
Twitching body
TREATMENT
❯ Behavioral therapies widely used for Tourette’s to expose the unpleasant feelings that precede the tic and encourage a response that stops it.
❯ Habit reversal training to teach use of incompatible behaviors in place of the tic, so planned intentional movements compete with the tic and prevent it.
❯ Lifestyle management such as relaxation techniques and listening to music to reduce frequency of tics.
❯ Antidepressants or anti-anxiety medication to support behavioral interventions if needed.
“The rhythm of music is very, very important for … patients with Tourette’s.”
This range of conditions affects a person’s ability to receive, send, process, and/or understand verbal, nonverbal, and visual concepts and may be apparent in hearing, language, and/or speech.
What are they?
The four main conditions are language, childhood fluency, speech-sound, and SCD (social communication disorders). They are often complex. Some are apparent in babies and toddlers, whereas others may not become obvious until a child is at school. The causes are wide-ranging. Communication disorders may develop of their own accord or stem from a neurological illness. They can be genetic—20–40 percent of children with a family history of speech and/or language impairment have communication disorders. Prenatal nutrition may be involved. Psychiatric disorders, ASD , Down syndrome, cerebral palsy, and physical problems including cleft lip or palate and deafness may limit a person’s ability to communicate.
How are they diagnosed?
To maximize a child’s development potential, early intervention is important; some conditions require lifelong management. A speech and language specialist takes a case history, including information about family background, medical conditions, and information from teachers and caregivers, to prepare a treatment plan.
CAUSES OF COMMUNICATION DISORDERS
More than one causal factor may be involved and the effects can range from mild to profound.
LANGUAGE DISORDER
The child does not understand others (receptive disorder) or cannot communicate thoughts (expressive disorder) or both (receptive-expressive disorder).
❯ Baby does not smile or babble in response to parents, and only has a few words by 18 months.
❯ Child does not play with others and prefers to be alone. May become shy and distant.
❯ Child has difficulty swallowing, affecting ability to speak.
CHILDHOOD FLUENCY
The child stammers or stutters, repeating words or parts of words, and prolonging speech sounds.
❯ Speech can become blocked as if child is out of breath.
❯ Child uses distracting sounds such as throat clearing or head and body movements to disguise their problem.
❯ Anxiety is increasingly evident as child tries to hide disorder.
❯ Child avoids public speaking as anxiety worsens the stutter.
SPEECH–SOUND DISORDER
The child has difficulty articulating sound patterns and mispronounces words beyond expected age range.
❯ Unclear speech, common in young children, continues beyond the age of eight.
❯ Child unable to produce correct sound patterns even though they can understand speech, so cannot make themselves understood by others.
❯ Limited understanding of rules of speech sounds is apparent.
SCD
The child cannot process verbal and visual information simultaneously.
❯ Child cannot adapt language to suit situation, so can be dogmatic, dominating, and inappropriate when talking to adults or peers.
❯ Child lacks nonverbal communication skills such as taking turns in conversation or other group activities.
❯ Child cannot greet people as they have little or no interest in social interaction.
IMPACT ON THE CHILD
Errors of thinking and communication affect daily interactions. Children become anxious, with low self-confidence.
❯ Developmental milestones are delayed as children learn through communication.
❯ Social isolation occurs because child does not initiate interaction and cannot make friends. May become target of bullies.
❯ Behavioral issues arise as child adopts avoidance techniques and may become aggressive if they cannot resolve speech difficulties.
SOCIAL COMMUNICATION DISORDER OR AUTISM SPECTRUM DISORDER?
SCD (social communication disorder) has many symptoms in common with ASD (autism spectrum disorder). Assessment must rule out ASD before doctors diagnose the child with SCD and establish a treatment plan.
Social communication disorder
Children with SCD find it difficult to learn the basic rules of conversation: how to start one, listen, phrase questions, stay on topic, and know when it is over. SCD can occur alongside other developmental issues such as language impairment, learning disabilities, speech-sound disorder, and ADHD
Autism spectrum disorder
Children with ASD find it hard to relate to people, emotions, and feelings. As with SCD, this can result in communication difficulties, impaired social skills, and altered sensory and visual perception. But ASD has an additional defining characteristic of restricted or repetitive behaviors.
TREATMENT
❯ Speech and language therapy essential to help language skills, speech-sound production and rules, fluency, and nonverbal gestures; for stutterers, support to control and/or monitor rate of speech and breathing.
❯ Positive behavior therapies to improve the relationship between behavior and communication.
❯ Family therapy, special educational support, and environmental adaptations to support language development.
An individual with this eating disorder persistently eats substances that are not food, such as dirt or paint. It can lead to serious complications if the substance is dangerous when ingested.
What is it?
Children and adults with pica may eat, for example, animal feces, clay, dirt, hairballs, ice, paint, sand, or metal objects such as paper clips. It is more common in children than adults—between 10 and 32 percent of children age 1–6 years are affected by pica. The odd eating behavior can create complications such as lead poisoning or intestinal damage from sharp objects. For a doctor to diagnose pica, the pattern of behavior must last for at least one month. After a medical examination to rule out causes such as nutrient deficiency or anemia as the root of the unusual cravings, a specialist health professional evaluates the presence of other disorders such as developmental disabilities or OCD .
RARER EATING DISORDERS
Irregular eating habits, eating unusual items, distress or avoidance around eating or mealtimes, or concerns about body weight or shape characterize eating disorders.
TREATMENT
❯ Behavioral therapies to associate healthy eating with positive reinforcement or reward. Positive behavior support to address aspects of family and home environment and minimize recurrence.
❯ Medication to enhance dopamine levels; supplements to remedy any nutrient deficiencies.
With this condition, a person regularly overeats to cope with low self-esteem and misery, although in fact the persistent, uncontrolled binge eating makes depression and anxiety worse.
What is it?
A person with binge-eating disorder regularly eats large amounts quickly when not hungry, alone or secretly, and feels shame and self-disgust after a binge. They feel they have no control over how much and how often they eat. Low self-esteem, depression, anxiety, stress, anger, boredom, loneliness, dissatisfaction with the body, pressure to be thin, traumatic events, and a family history of eating disorders are all factors that increase the risk of developing it. The disorder can also develop after the person follows such a strict diet that they are left very hungry and have food cravings. It is the most common eating disorder in the US. A GP may diagnose the disorder from the person’s weight gain—the most common physical effect.
Bingeing cycle
People with a bingeeating disorder are using food as an instant, albeit negative, way to relieve emotional pain instead of finding positive methods of tackling the underlying cause. The result is a perpetual cycle of eating, relief, depression, and yet more eating.
Anxiety rises and depression sets in as eating provides only short-lived “pain” relief.
Relief from increasingly distressing feelings comes only with thoughts of food.
The need to eat to relieve depression grows in urgency; the person plans a binge, often buying special foods for that purpose.
The person eats large amounts of food rapidly (regardless of degree of hunger), often in secret, may be in a dazed state while eating, and may feel uncomfortably full afterward.
Anxiety drops as eating temporarily numbs the feelings of stress, sadness, or anger.
Low mood returns with self-disgust because of the guilt and shame associated with binge eating.
TREATMENT
❯ Psychotherapy in groups or one-on-one.
❯ Self-help programs through books, in online courses, as part of a support group, or supervised by a health professional.
A serious eating disorder, bulimia is characterized by a person controlling their weight through severely restricting intake, then binge eating and purging the body of the food.
What is it?
People with bulimia have an abnormal fear of putting on weight and so become obsessed with food and dieting. Unlike those with anorexia , they are usually at or near a normal weight for their height and build. However, like a person with anorexia, they have a distorted self-image and believe they are too fat. A person with bulimia may often appear tense or anxious and behave furtively, rapidly consuming large amounts of food in secret before disappearing to the bathroom to make themselves vomit. This behavior is a mechanism for coping with life events—although in fact it makes daily living a struggle—and is linked to depression, anxiety, and social isolation. Pressure to conform to body shapes promoted by the fashion and beauty industries and a family history of bulimia increase the risk. Bulimia is more common in females, but incidence in males is rising. Puberty and selfconsciousness are often triggers, and boys and girls in their teens are especially vulnerable to bulimia if teased as an overweight child. Bulimia can cause irreversible damage to the heart, bowels, teeth, and fertility. Treatment depends on the severity of the condition, and recovery can be a long process.
Binge−purge cycle
The person has a low self-opinion and sees losing weight as a way of gaining selfworth. They may also exercise fanatically to burn off the additional calories and avoid social occasions that involve food.
Causes
❯ The individual may have a caregiver who thinks looks are important and criticizes their weight or appearance.
❯ The person may want to take control of an aspect of their lives, particularly if recovering from a traumatic event.
❯ Images of celebrities with flawless, thin bodies trigger the start of a strict diet.
❯ Despair sets in when the person cannot keep to the diet.
Physical effects
❯ Frequent weight gain and loss.
❯ Bad breath, stomach pain, sore throat, and damaged tooth enamel from acid levels in vomit.
❯ Dry skin and hair, hair loss, brittle nails, lethargy, and other signs of poor nutrition.
❯ Heart strain, hemorrhoids, and weak muscles from misuse and overuse of laxatives and diuretics.
❯ Irregular/absent periods in females.
❯ Feeling bloated and/or constipated.
❯ Calluses on the back of hands from induced vomiting.
PEOPLE WITH BULIMIA feel as if they have no control over eating habits, which increases their fear of weight gain.
TREATMENT
❯ Psychotherapies such as group therapy, self-help, or one-on-one cognitive behavioral therapy or interpersonal therapy.
❯ Antidepressants prescribed along with therapy.
❯ In-patient treatment needed in extreme cases.
1.5% of American women have or have had bulimia in their lifetime
With this serious emotional disorder, a person wants to weigh as little as possible. They develop an aversion to food and their appetite reduces as they eat less and less.
What is it?
A person with anorexia becomes so afraid of gaining weight that they cannot eat normally. They may take appetite suppressants, laxatives, or diuretics (to remove body fluid), or make themselves vomit after meals (bulimia nervosa, pp.92−93), but they may also binge (binge-eating disorder, p.94). Many factors can trigger anorexia. Pressures at school, such as exams or bullying (particularly if the focus is on body weight or shape), can contribute, as can occupations such as dancing or athletics where being thin is considered “the ideal.” The disorder can also be a response to stress in childhood or lack of control over life events, such as losing a job, relationship breakdown, or bereavement, which makes the person exert excessive control over internal processes that are within their power. Anorexia affects more females than males. Many of those who develop it share personality and behavioral traits. They are often emotionally controlled, have a tendency toward depression and anxiety, find it difficult to handle stress, and worry excessively. Many individuals set themselves strict, demanding goals. They may have feelings of obsession and compulsion, but not necessarily OCD . Living withanorexia can make it hard to maintain relationships. It can also have an irreversible impact on the body and cause infertility or serious pregnancy complications.
How is it diagnosed?
The GP, clinical psychologist, or specialist health professional asks the individual questions about their personal and family history, weight, and eating habits. The person needs treatment as early as possible to reduce the risk of complications. In most cases, the treatment plan involves psychotherapy and individually tailored advice on eating and nutrition. Recovery can take years.
Symptoms of anorexia
All symptoms relate to self-esteem, body image, and feelings, and divide into three main categories: cognitive (feelings and thoughts), behavioral, and physical.
Cognitive symptoms
❯ Expresses a fear of gaining weight and becomes obsessed with body shape.
❯ Believes that being thin is good and is convinced that they are overweight.
❯ Measures self-worth in terms of body weight and shape.
❯ Obsesses about food and the perceived negative consequences of eating.
❯ Becomes irritable, moody, and unable to concentrate (partly due to hunger), which impacts school or work.
Behavioral symptoms
❯ Behaves obsessively around food and diets, and counts calories excessively. Avoids “fatty” foods and/or eats only low-calorie foods. May skip meals.
❯ Avoids eating in front of others, and/or purges after eating.
❯ Lies about how much they eat.
❯ Repeatedly weighs themselves or checks their body shape in the mirror.
❯ Exercises obsessively.
❯ Becomes socially withdrawn.
Physical symptoms
❯ Obvious weight loss.
❯ Irregular or absent periods in females.
❯ Poor dental health and smelly breath due to persistent vomiting.
❯ Soft, fine, “downy” hair growing on the body, while head hair falls out.
❯ Has difficulty sleeping but is very tired.
❯ Is weak, light-headed, and dizzy.
❯ Has stomach pains, and is constipated and bloated.
❯ Has swollen hands and feet.
TREATMENTS
❯ Multidisciplinary care team, including a GP, psychiatrists, specialist nurses, and dietitians to ensure that a person gains weight safely and to support family and close friends.
❯ Cognitive behavioral therapy to help the person understand and explain their problem and see it as a cycle of triggers, thoughts, feelings, and behaviors. Therapist and patient collaborate on interventions that break the chain of thoughts maintaining anorexia.
❯ Cognitive analytic therapy to examine the way the person thinks,feels, and acts, as well as the events and relationships that underlie their past experiences—often in childhood.
❯ Interpersonal therapy to resolve problems with attachment and relating to other people.
❯ Focal psychodynamic therapy to explore how early-childhood experiences may have affected the person.
❯ In-patient treatment for severe cases; supervised weight gain through strict daily routines and eating plans, often including group therapy for peer support.
This is an often short-term, dissociative disorder in which a person becomes separated from their personal memories following stress, trauma, or illness.
What is it?
Dissociative amnesia is often linked to overwhelming stress, such as witnessing or suffering from abuse, an accident, or a disaster. The resulting severe memory loss often affects specific recollections, such as a certain period during childhood, or something associated with a friend, relative, or peer. Alternatively, the amnesia may focus on a traumatic event, for example, a crime victim may have no memory of being robbed at gunpoint, but can recall details from the rest of that day. A person may develop generalized memory loss and may not remember their name, job, home, family, and friends. They may disappear and be reported missing. They might even create a totally new identity, fail to recognize people or places from their past life, and be unable to explain themselves—this is known as a dissociative fugue. Clinical diagnosis will involve completing assessment questionnaires that help identify a trigger and enable the individual to capture and rate their symptoms. Physical checks and psychological examinations are also carried out to exclude other medical causes of memory loss.
Memory recovery
Most cases of dissociative amnesia are shortterm, and while memories may temporarily fall away, they often return suddenly and completely. The recovery may happen on its own, after being triggered by something in the person’s surroundings, or in a therapy session.
TREATMENT
❯ Psychotherapies, such as cognitive behavioral therapy, dialectical behavior therapy, eye movement desensitization and reprocessing, family therapy, and art therapies such as hypnosis or mindfulness meditation can help the person understand and deal with the stress that triggered the disorder, and learn coping strategies .
❯ Medication, such as antidepressants, may be prescribed for the depression or psychosis that can be associated with the amnesia .
These are two related dissociative disorders. Depersonalization makes a person feel disconnected from their thoughts, feelings, and body, whereas derealization makes them feel disconnected from their environment.
What are they?
The feelings that result from these two conditions can be very disturbing and seriously interfere with a person’s ability to function. Some people fear they are going mad, or become depressed, anxious, or panicky. People with depersonalization describe feeling like a robot and not in control of their speech or movement, as if they are an outside observer of their own thoughts or memories. They may also feel that their body is distorted. With derealization a person can feel alienated and disconnected from their surroundings. In some, the symptoms for these disorders are mild and short-lived, whereas in others they may persist for months or even years. Little is known about what causes these disorders, but biological and environmental factors may play a role. Some people appear to be more prone to them, because they are neurologically less reactive to emotions or they may have a personality disorder (pp.102–107). The disorders can be triggered by intense stress, trauma, or violence. If symptoms are present, a clinical assessment will include a full medical history and physical examination to rule out illness or side effects of medication, and questionnaires will be completed to identify associated symptoms and possible triggers. An individual is diagnosed with depersonalization and/or derealization disorder only when they persistently or repeatedly suffer from distorted perceptions of detachment from themselves or their environment. Many people experience a temporary feeling of dissociation from their thoughts or surroundings at some point in their lifetime, but fewer than 2 percent of people will be identified as having one, or both, of these disorders.
Out-of-body experience
A person can be so dissociated from reality that they feel as if they are observing themselves in a movie and cannot relate to the individual in the real world.
TREATMENT
❯ Psychotherapies, particularly cognitive behavioral therapy , psychodynamic therapy , or mindfulness meditation can help a person understand why the feelings occur, learn coping strategies to manage the situations that trigger them, and gain control over symptoms.
❯ Medication, such as antidepressants , can be prescribed to treat any associated disorders, including anxiety and depression.
In this rare and severe condition, a person’s identity is fragmented into two or more distinct personality states. The parts do not join up into a whole.
What is it?
A person with DID has a splintered identity, rather than a growth of separate personalities, which is why the name of the condition was changed from its previous term of multiple personality disorder. The individual feels as though they have different people within (called alters). Each alter has its own persona, with its own pattern of thinking and communicating, even down to different handwriting and physical requirements, such as wearing glasses. Someone with DID finds it hard to define what they are like, and may refer to themselves as “we.” They have no control over when and which alter takes over, and for how long.
Dissociative experiences
An individual with DID uses dissociation—disconnection from the world around them—as a defense mechanism. They may feel as if they are floating away, watching themselves from outside. As if in a movie, the person observes rather than feels their emotions and parts of their body. The world around a person affected by DID may seem unreal and hazy, with objects changing appearance. The individual has significant and frequent gaps in memory, unable to recall personal information in a way that is more extreme than forgetfulness. They may not remember people, places, and events in their lives from the distant and recent past, yet vividly relive other things that have happened. The person has moments of absence while carrying out day-to-day activities and may travel somewhere but be unable to remember how they got there. The person regularly experiences symptoms of personality change and dissociation. These symptoms are thought to be a way of coping that often goes back to severe and prolonged trauma experienced in childhood, but the dissociation disrupts everyday life long after the trauma has ceased. Affected individuals continue to use the dissociation as a way of coping in all stressful situations in later life.
How is it diagnosed?
If a specialist suspects DID, they will complete mental health questionnaires that capture and rate the person’s symptoms. The aberrant and inexplicable behavior that characterizes DID is distressing and confusing for the individual and impacts negatively on work, social life, and intimate relationships. DID often exists alongside anxiety and depression, panic attacks, OCD , hearing voices, and suicidal feelings.
Identity alteration
Each alter, as the identity fragments of someone with DID are called, has distinct patterns of perception and personality that recur and take control of the individual’s behavior. Typically the personalities know each other and communicate, sometimes criticizing one another. The transition from one to another is sudden and the person has no control over which one is in charge, but certain stressors can make a particular alter emerge.
SWITCHING BETWEEN ALTERS
Different name can denote a switch to the thinking patterns of another alter.
Different appearance, for example, hair color or clothing style, can change the host’s persona
The host identity is the one main alter that a person may feel is most like them. This host identity may not remember facts about their personal history when a different alter is in control.
Change of role can enable a view of life events from another standpoint.
Another gender or age changes memories or perceptions of events.
Opposing attitude from the host’s Identity provide a different prospective on life events
A younger self may talk like a childlike way or even be unable to talk
8−13 the typical number of identities in people with dissociative identity disorder
A person with pyromania sets fires purposely. This very rare impulse-control disorder is triggered by stress, and the action provides relief from tension or distress.
What is it?
Also known as firesetting, pyromania is an obsessive desire to light fires. It can be a chronic (long-term) problem, or restricted to several occurrences during a period of unusual stress. A person with pyromania is excessively fascinated with making fires and situations involving fire, as well as witnessing or assisting in the fire’s aftermath. Individual factors that contribute to pyromania may include antisocial behaviors and attitudes, sensation and/or attention seeking, lack of social skills, and inability to cope with stress. Parental neglect or emotional detachment, parental psychological disorders, peer pressure, and stressful life events can all be triggers in both children and adults. Interviews with affected children and teens often identify a chaotic household, in which case a whole-family approach to treatment is required .
PYROMANIA IN CHILDREN, TEENS, AND ADULTS
❯ In children and teens firesetting may be a cry for help, or part of a larger pattern of aggression. Teens may be influenced by antisocial adults in their community. Some are diagnosed with psychotic or paranoid disorders , and others may be cognitively impaired.
❯ In adults pyromania has been linked to symptoms that include depressed mood, thoughts of suicide, and poor interpersonal relationships. It is often associated with psychological problems such as OCD .
Destructivecycle
The cycle of obsession and gratification is difficult to break.
Fire, its aftermath, and fire-related equipment and personnel fascinate the person.
Tension builds up, leading to a strong desire to light a fire.
Lighting the fire gratifies overwhelming urge.
Feelings of euphoria and relief result from seeing the fire.
TREATMENT
❯ Cognitive and behavioral therapies tailored to children to include problemsolving and communication skills, anger management, aggression replacement training, and cognitive restructuring; long-term, insight-oriented psychotherapy for adults.
An individual with kleptomania has an irresistible and repeated compulsion to steal items. These episodes of stealing occur unexpectedly, without planning.
What is it?
A person with kleptomania steals on impulse and often throws the stolen goods away, because they are mostly interested in the act of stealing. Kleptomania is distinguished from shoplifting in that most shoplifters plan the theft, usually because they want an item but do not have enough money to buy it. Many people with kleptomania live secret lives of shame because they are afraid to seek help; up to 24 percent of those arrested for shoplifting are thought to suffer from it. Kleptomania is associated with other psychiatric problems such as depression, bipolar disorder, generalized anxiety disorder, eating and personality disorders, substance abuse, and other impulse-control disorders. There is evidence to link kleptomania with the neurotransmitter pathways associated with behavioral addictions and mood-enhancing neurochemicals like serotonin. There is no specific cure for kleptomania, but psychotherapy and/or medication may help break the cycle of compulsive stealing.
Perpetual pattern
A person with kleptomania may report feeling tense before they steal, then pleased and gratified as they do it. The subsequent guilt can increase the tension again.
Intrusive thoughts about stealing triggered.
Urge to steal is impossible to resist.
Stealing Item is often not for personal use.Item is usually hidden or thrown away.Item may have no monetary value.
Arousal and relief follow immediately after the event.
Feelings of stress, guilt, and selfloathing arise.
Also known as compulsive gambling, this is an impulse-control disorder that exists when a person repeatedly gambles despite the significant problems or distress it causes themselves and others.
What is it?
The thrill of winning releases dopamine from the reward center in the brain. For some people the act of gambling becomes addictive and they need ever bigger wins to achieve the same thrill. Once a gambling disorder takes hold, the cycle is difficult to break. The disorder may start from desperation for money, the need to experience the highs, the status associated with success, and the atmosphere of a gambling environment. The person can become irritable if they attempt to cut down, and then may gamble because of the distress. Severe disorders can take hold through a financial desperation to recoup lost money. Even when the person finally wins again, it is rarely enough to cover losses. Aside from significant financial loss, excessive gambling can impact badly on relationships. It can also cause anxiety, depression, and suicidal thoughts. Physical signs can include sleep deprivation, weight gain or loss, skin problems, ulcers, bowel problems, headaches, and muscle pains. Because most people do not admit they have a problem, a major component of treatment is helping them to acknowledge it. The true prevalence of the disorder is not known because so many hide their habit.
TREATMENT
❯ Cognitive behavioral therapy to help people learn to resist the beliefs and behaviors that maintain the disorder.
❯ Psychodynamic therapy to help grasp the meaning and consequences of the behavior.
❯ Self-help groups and counseling to help understand how the behavior affects others.
1%of the American population are pathological gamblers
control disorders are diagnosed in people who cannot withstand the urge to perform problematic behaviors. In addiction, a pleasurable activity becomes compulsive and interferes with daily life.
What are they?
The basic concepts underlying impulsive and addictive behaviors overlap. Some psychologists think that impulse-control disorders should be classed as addictions. In impulse-control disorders, a person perpetuates their behavior regardless of the consequences, and they become less and less able to control their inner urges. Usually, a person feels an increasing tension or arousal before the action, pleasure or relief while doing it, and regret or guilt in the aftermath. Environmental and neurological factors both play a part in the development of the disorders and they may be triggered by stress. The recognized impulse-control disorders are compulsive gambling (opposite), kleptomania (p.84), pyromania (p.85), hair pulling (p.60), and intermittent explosive disorder (below). Sex, exercise, shopping, and Internet addictions (below) share similar traits.
This is a serious condition in which the use of alcohol or drugs, or both, leads to physical and psychological problems that affect the individual’s working or home life for the worse.
What is it?
Also known as drug use disorder or substance abuse, this condition can cause wide-ranging impairments and psychological distress. Symptoms and signs of substance abuse (whether alcohol or drugs) include taking drugs regularly, maybe daily, to function; taking drugs even when alone; continuing to use drugs even when the person knows it is harming their own health, family, or work; making excuses to use drugs and reacting with aggression to inquiries about their substance use; being secretive about using drugs; losing interest in other activities; impaired ability to work; neglecting to eat or attend to physical appearance; confusion; lethargy; depression; financial problems; and criminal activity such as stealing money. In the longer term, overconsumption of alcohol can cause weight gain and high blood pressure and increase the risk of depression , liver damage, problems with the immune system, and some cancers. Drugs can be associated with mental health issues such as depression, schizophrenia , and personality disorders . Alcohol or drug abuse usually begins as a voluntary behavior, encouraged or tolerated within the person’s social and cultural climate. Peer pressure, stress, and family dysfunction can escalate the problem. A child with a family member who has chemical-dependency issues may be at a higher risk of the disorder for either environmental or genetic reasons or both.
How is it diagnosed?
Diagnosis begins with the person recognizing that they have a problem; denial is a common symptom of addiction. Empathy and respect are more likely to induce a person to accept that they have substance use disorder than orders and confrontation. The GP or specialist grades the person’s behavior (below) while the individual is using the substance.
Behavior patterns
The diagnosis of this disorder, whatever the substance, is based on a set of 11 behaviors related to its use. The severity of the disorder is based on how many of these behaviors are present: 0–1 = no diagnosis; 2–3 = mild substance use disorder; 4–5 = moderate substance use disorder; 6+ = severe substance use disorder.
Impaired control
❯ 1. Uses substance for longer and/or in larger amounts than originally intended.
❯ 2. Wants to cut down, but cannot do so.
❯ 3. Spends longer and longer getting, using, and recovering from using the substance.
❯ 4. Has intense cravings for the substance, which makes it difficult for the person to think about anything else.
Social impairment
❯ 5. Continues to use despite knowing the problems it causes with life at home or work.❯ 6. Continues to use despite arguments with family or the loss of friendships it causes.
❯ 7. Gives up social and recreational activities as a result, so spends less time with friends and family, and becomes increasingly isolated.
Risky use
❯ 8. While under theinfluence, engages in risky sexual behavior or puts themselves or others in danger, for example, by driving, operating machinery, or swimming.
❯ 9. Continues to use while aware that the substance is making psychological or physical problems worse (for example, drinking even when liver damage has been diagnosed).
Pharmacological criteria
❯ 10. Becomes tolerant to the substance, so needs increasing amounts to achieve the same effects. Different drugs vary in terms of how quickly tolerance develops.
❯ 11. Suffers withdrawal such as nausea, sweating, and shaking if the intake is stopped.
29.5million people in the world have drug use disorder
United Nations Office on Drugs and Crime, World Drug Report 2017
Also known as post-concussion syndrome, this is a degenerative condition of the brain characterized by physiological and psychological disturbances following closed head injuries.
What is it?
CTE is most often seen in service personnel or people who take part in high-impact contact sports, such as football, rugby, or boxing, and there is no cure. Physical symptoms include headache, dizziness, and pain. Psychological symptoms are memory loss, confusion, impaired judgment, impulse-control problems, and even hallucinations. An individual may become aggressive and have difficulty maintaining relationships. Signs of Parkinson’s and dementia can emerge later. The disturbances may develop early, or emerge years after the head trauma. A preventive approach is advisable, with the use of protective headgear and the introduction of rules that disallow contact above chest or shoulder height in sport. At the moment it is possible to diagnose CTE only after death. Tests, brain scans, and biomarkers are being developed to help identify the condition earlier.
Cumulative effect of head injury
Multiple blows to the unprotected skull can lead to irreversible injury. In a study of 100 people with mild head injury, 20–50 showed symptoms of CTE three months after the initial injury, and about 1 in 10 still had problems a year later.
1.A blow to a healthy brain can cause concussion but a person is likely to recover completely.
2.The initial injury can leave a vulnerability, so the brain is less able to recover from a second one.
3.After three or more blows the brain is more susceptible to widespread, permanent damage.
CTE was identified in 99% of former US National Football League players
This is an (as yet) incurable, degenerative disorder, also known as mild or major neurocognitive impairment. It is characterized by memory disorders, personality changes, and impaired reasoning.
What is it?
The term dementia describes a set of symptoms that affect the brain and gradually become more severe. Symptoms include difficulties with concentration, problem solving, carrying out a sequence of tasks, planning, or organizing, as well as general confusion. A person with dementia may lose track of days or dates, and find it hard to follow a conversation or recall the right word for something. They may also be unable to judge distances or see objects in three dimensions. Dementia may cause people to feel insecure and lose their self-confidence and can result in depression. Many different conditions, such as Alzheimer’s, cardiovascular disease, Lewy bodies, and disorders of the front and side lobes of the brain, cause the symptoms.Dementia is mainly seen in older adults, but can occur in people in their 50s (known as early onset), and sometimes even younger. There is no single assessment for dementia. The GP uses memory and thinking tests and may order a scan to confirm which areas of the brain are damaged. Treatment aims to alleviate symptoms and slow their progression.
CAUSES
❯ Alzheimer’s disease causes abnormal proteins to build up around brain cells and damage their structure. This disrupts the chemical messages that pass between the cells so the cells gradually die. Symptoms progress as more parts of the brain are affected.
❯ Vascular dementia can result from cardiovascular disease. It occurs when blood flow to the brain is impaired (for example, by a stroke), causing problems with reasoning, planning, judgment, and memory.
❯ Mixed dementia results when Alzheimer’s and vascular dementia occur at the same time.
❯ Dementia with Lewy bodies has similar symptoms to Alzheimer’s and Parkinson’s disease. Also known as Pick’s disease, it occurs when protein bodies form in nerve cells and often causes hallucinations and delusions.
❯ Frontotemporal dementia is a rarer form that affects the temporal (side) and frontal lobes of the brain. It alters personality and behavior, and makes use of language difficult.
How it affects a person
Because every person is different, their experience of dementia is, too. The diagnosis is based on a person’s history and how the symptoms affect their ability to cope day to day.
PEOPLE WITH DEMENTIA feel insecure, lose confidence in themselves, and need help preparing for the road ahead.
TREATMENT
❯ Cognitive stimulation and reality orientation therapy for short-term memory.
❯ Behavioral therapy to help carry out daily routines.
❯ Validation therapy—the main caregiver reading out loud, respectful statements.
❯ Cholinesterase inhibitors to boost memory and judgment.
This is a very rare form of psychosis that causes a person to experience complex and often disturbed thoughts and delusions that are not true or based on reality.
What is it?
Previously known as paranoid disorder, delusional disorder is marked by an individual’s inability to distinguish what is real from what is imagined. The delusions may be misinterpretations of experienced events, and are either not true or highly exaggerated. They may be nonbizarre and relate to situations that could occur, such as being followed, poisoned, deceived, or loved from a distance, or may be bizarre delusions that are impossible, for example, a belief in an imminent alien invasion.Delusional disorder can make it hard for a person to concentrate, socialize, and live a normal life, because it can cause dramatic changes in a person’s behavior that result in conflict with those around them. Individuals may become so preoccupied with their delusions that their lives are disrupted. However, others continue to function normally and, apart from the subject of their delusion, do not behave in an obviously odd manner. Some people experience hallucinations— seeing, hearing, tasting, smelling, or feeling things that are not really there.Psychological disorders known to trigger delusional episodes include schizophrenia , bipolar disorder , severe depression or stress, and lack of sleep. General medical conditions that can cause them are HIV, malaria, syphilis, lupus, Parkinson’s, multiple sclerosis, and brain tumors. Misuse of substances such as alcohol or drugs can also trigger delusional episodes in some people.
How is it diagnosed?
A doctor will first take a complete medical history of the individual. They will ask about symptoms and will want to know how a delusion affects a person’s day-to-day functioning, any family history of mental health conditions, and details of medications and/or illegal substances a person has been taking.
Thematic delusions
Delusions are fixed beliefs that do not change, even when a person is presented with conflicting evidence, and characteristically follow particular themes (right). Individuals are likely to display the delusion for a month or longer, and most do not admit they are problematic. The person may appear completely normal as long as an outsider does not touch on the belief.
Somatic A person with these delusions has physical or bodily sensations—for example, as a result of believing insects are crawling under their skin.
Erotomanic A delusion in which a person believes that another individual, often someone famous, is in love with them; may lead to stalking behavior.
Grandiose An individual with grandiose delusions believes they have a great unrecognized talent or knowledge, for example, they may be a special messenger, guru, or God.
Persecutory A person with these delusions feels that they are being persecuted or mistreated—for example, stalked, drugged, spied on, or the victim of slander.
Jealous People with this delusion have a morbid but unfounded belief that their partner has been unfaithful or is deceiving them.
Mixed or unspecified
Themes are said to be mixed Jealous People with this delusion have a morbid but unfounded belief that their partner has been unfaithful or is deceiving them. if several types of delusions are present but no particular one predominates. In some cases the delusion does not fall into any of the main categories and is unspecified.
TREATMENT
❯ Medication prescribed may include antipsychotic drugs to reduce the delusional symptoms and antidepressants such as selective serotonin reuptake inhibitors (SSRIs) to help with the depression that can be associated with the disorder.
❯ Psychotherapies such as cognitive behavioral therapy to help examine the strongly held beliefs and support changes needed.
❯ Self-help groups and social support to reduce the stress that results from living with this disorder and to help those around them, and family, social, and/or school intervention to help develop social skills to reduce the impact of the disorder on quality of life.
An episodic condition that affects both behavior and motor skills, catatonia is characterized by abnormal psychomotor functioning and extreme unresponsiveness when awake.
What is it?
Catatonia is a state of immobility that can persist for days or weeks. Those with the condition may have an extremely negative outlook and may not respond to external events, become agitated, have difficulty speaking due to extreme anxiety, and refuse to eat or drink. Symptoms also include feelings of sadness, irritability, and worthlessness, which can occur nearly every day. An individual may lose interest in activities, lose or gain weight suddenly, have trouble getting to sleep or out of bed, and feel restless. Decision making is impaired and suicidal thoughts are common. This condition can have a psychological or neurological cause, and may be associated with depression or psychotic disorders. It is estimated that 10−15 percent of people with catatonia also have symptoms of schizophrenia , while about 20−30 percent of individuals with bipolar disorder may experience catatonia during their illness—mostly during their manic phase.
Diagnosing catatonia
A mental health professional observes an individual and looks for a number of symptoms. At least 3 out of the 12 symptoms described (right) must be present to confirm a diagnosis of catatonia.
Mutism Silent and apparently unwilling or unable to speak.
Echolalia Constantly repeats what other people have said.
Grimacing Makes distorted facial expressions that show disgust, dislike, and even pain
Stupor Immobile, lacks expression, and does not respond to stimuli.
Catalepsy May be rigid, have a seizure, or be completely unresponsive in this trancelike state.
Waxy flexibility Limbs can be moved by someone else and will remain in the new position.
Agitation Movement may be purposeless and risky.
Mannerism Strikes poses or makes idiosyncratic movements.
Posturing Moves from one unusual position to another.
Negativism Resistant to any outlook other than a negative one.
Echopraxia Constantly mimics other people’s movements.
TREATMENT
❯ Medication prescribed depends on the symptoms, but includes antidepressants, muscle relaxers, antipsychotics, and/or tranquilizers such as benzodiazepines, but these carry a risk of dependency . Outside help is needed to ensure compliance with medication and to teach living skills.
❯ Electroconvulsive therapy may be used when medication is ineffective. This involves transmitting an electric current through the person’s brain .
This is a long-term mental health condition in which a person suffers both the psychotic symptoms of schizophrenia and the deregulated emotions that characterize bipolar disorder at the same time.
What is it?
While symptoms may vary from person to person, one episode will feature both psychotic and mood symptoms (manic, depressive, or both) for part of the time and a period with only psychotic or mood symptoms for most of the time over a period of at least two weeks. Schizoaffective disorder can be triggered by traumatic events that took place when a person was too young to know how to cope or was not being cared for in a way that made it possible to develop coping skills. Genetics may play a part, too. It is more common in women and usually begins in early adulthood. A mental health professional will assess the symptoms and will want to know how long they have been present, and what triggers them. This chronic condition impacts every aspect of a person’s life, but symptoms can be managed. Family interventions to raise awareness of the disorder can improve communication and support.
The different forms
People with this disorder experience periods of psychotic symptoms—such as hallucinations or delusions—with mood disorder symptoms of either a manic type or a depressive type, but sometimes both. The condition features cycles of severe symptoms followed by periods of improvement.
Mood disorder symptoms
Manic type is hyperactive, feels high, cannot sleep, and takes risks.
Depressive type feels sad, empty, and worthless, even suicidal.
Mixed type has symptoms of both depression and mania.
TREATMENT
❯ Medication is needed long-term; usually combinations of mood stabilizers plus antidepressants for depressive types or antipsychotics for manic types .
❯ Cognitive behavioral therapy can help a person make links between thoughts, feelings, and actions; learn the cues preceding behavior change; sand develop coping strategies.
1%of the population is likely to develop schizoaffective disorder
This is a long-term condition that affects the way a person thinks. It is characterized by feelings of paranoia, hallucinations, and delusions, and significantly impacts a person’s ability to function.
What is it?
The word schizophrenia comes from the Greek, and literally means “split mind,” which has led to the myth that people with the condition have split personalities, but they do not. Instead they suffer from delusions and hallucinations that they believe are real. There are different types of schizophrenia. The main ones are paranoid (hallucinations and delusions); catatonic (unusual movements, switching between being very active and being very still); and disorganized, which has aspects of both. Despite popular belief, individuals with schizophrenia are not always violent. They are, however, more likely to abuse alcohol and drugs, and it is these habits, combined with their condition, that can cause them to become aggressive. Schizophrenia appears to result from a combination of physical, genetic, psychological, and environmental factors. MRI scans have identified abnormal levels of neurotransmitters dopamine and serotonin and unusual brain structure, and there might be a correlation between the condition and pregnancy or birth complications. It is also thought that excessive cannabis use in young adulthood can be a trigger.Popular theories regarding the causes of schizophrenia in the second half of the 20th century included family dysfunction theories, such as the “double bind” (when people are faced with contradictory, irreconcilable demands for courses of action), high levels of parent/ caregiver “expressed emotion” (not tolerating those with the disorder), and learning the schizophrenic role through labeling. Since then, mental health specialists have observed that hearing voices or feeling paranoid are common reactions to trauma, abuse, or deprivation. Stress can trigger acute schizophrenic episodes, and learning to recognize their onset can help with management of the condition.
Symptoms of schizophrenia
These are classified as positive or negative. Positive symptoms are psychotic additions to an individual, whereas negative symptoms can look like the withdrawal or flat emotions seen with depression. Schizophrenia is likely if a person has experienced one or more symptoms from both domains for most of the time for a month.
Positive symptoms (psychotic)
These symptoms are classed as positive because they are additions to a person’s mental state and represent new ways of thinking and behaving that only develop with the condition.
❯ Hearing voices is common, and can occur occasionally or all the time. The voices may be noisy or quiet, disturbing or negative, known or unknown, and male or female.
❯ Hallucinations involve seeing things that are not there but seem very real to the person, and are often violent and very disturbing.
❯ Feeling sensations can cause a person to be convinced that they have unpleasant creatures such as ants crawling on or under their skin.
❯ Smelling and tasting things that cannot be identified can arise, and there may be difficulty discriminating between smells and tastes.
❯ Delusions—fixed beliefs—are held despite evidence to the contrary. The person may think they are famous and/or being chased or plotted against.
❯ Feelings of being controlled by, for example, a religious or dictatorial delusionist, can overwhelm a person. The beliefs can make them act differently.
Negative symptoms (withdrawal)
These symptoms are called negative because they represent a loss of certain functions, thoughts, or behaviors that a healthy person exhibits, but that are absent in those with schizophrenia.
❯ Difficulty communicating with others can result in changed body language, a lack of eye contact, and incoherence.
❯ “Flattened” emotions result in a significantly reduced range of response. The person will take no pleasure in activities.
❯ Tiredness may result in lethargy, change in sleep patterns, staying in bed, or sitting in the same place for long periods.
❯ Absence of willpower or motivation makes it difficult or even impossible for a person to engage in normal day-to-day activity.
❯ Poor memory and concentration means that the individual is unable to plan or set goals and has difficulty keeping track of thoughts and conversations.
❯ Inability to cope with everyday tasks results in disorganization. The individual stops looking after themselves, domestically or personally.
❯ Becoming withdrawn from social and community activities can disrupt the individual’s social life.
TREATMENT
❯ Community mental health teams such as social workers, occupational therapists, pharmacists, psychologists, and psychiatrists work together to develop ways to help a person stay stable and progress
❯ Medication in the form of antipsychotics is prescribed to reduce mostly positive symptoms, but it does not cure the condition.
❯ Cognitive behavioral therapy and the technique of reality testing can help with management of symptoms such as delusions. New developments use imagery to defuse stress that negative symptoms cause.
❯ Family therapy can improve relationships and coping skills within the family and educate anyone involved in a person’s care.
Around 1.1% of the global adult population has schizophrenia
ASD describes a spectrum (range) of lifelong disorders that affect a person’s ability to relate to other people—and their emotions and feelings—making social interaction difficult.
What is it?
ASD is generally diagnosed in childhood and can present in a variety of ways. A parent or caregiver may notice that a baby does not use vocal sounds or an older child has problems with social interaction and nonverbal communication. Symptoms such as repetitive behaviors, problems talking, poor eye contact, tidying or ordering rituals, bizarre motor responses, repetition of words or sentences, a restricted repertoire of interests, and sleep problems are common. Some children with ASD may also have depression or ADHD Genetic predisposition, premature birth, fetal alcohol syndrome, and conditions such as muscular dystrophy, Down syndrome, and cerebral palsy are known to be associated with ASD. A GP first examines the child to rule out physical causes for the symptoms, then refers them for specialist diagnosis. Information is gathered about all aspects of the child’s behavior and development, at home and school. There is no cure, but specialized therapies such as speech therapy and physical therapy can help. One in every 68 people in the US has ASD and it is identified in more girls than boys.
HIGH-FUNCTIONING AUTISM AND ASPERGER’S
High-functioning autism (HFA) and Asperger’s syndrome (AS) are both terms that are applied to people with characteristics of ASD, but who are of above average intelligence with an IQ of more than 70. However, they exist as two separate diagnoses, as those with HFA have delayed language development, which is not present in AS. Diagnosis of HFA or AS may be missed in children as they are socially awkward with a manner that is not easily understood. The ASD traits theyshare of perfectionism and obsessive interest in a specific subject can mean that they become experts in their area of interest. Like ASD, those with HFA or AS also require strict routines and have sensitivities to certain stimuli, awkwardness, and difficulty behaving appropriately and communicating in social situations; the severity of these symptoms will differ in each individual. Long-term difficulties arise with social and intimate relationships, both at school and into adulthood.
Degrees of ASD
ASD manifests itself in different ways and to different degrees in each person. Autistic author and academic Stephen M. Shore said, “If you’ve met one individual with autism, you’ve met one individual with autism.”
Communication
Problems with language are common. Some people with ASD are fluent, while others are speech impaired. All tend to be literal and have difficulty with understanding humor, context, and inference.
Social interaction
Impaired social skills mean that a person with ASD cannot recognize another’s personal space or read body language. The person might think out loud or repeat what another person has said.
Repetitive behavior
Repetitive behavior traits are common. An individual may make repetitive movements such as hand flapping or rocking, or develop rituals such as lining up certain toys or flicking switches on and off
Sensory skills
Heightened sensitivity to sound can cause a person to develop avoidance behaviors such as humming, covering their ears, or self-isolation in a preferred space to escape noise.
Motor skills
Difficulties with movement, such as coordination and motor planning, are common in children with ASD. Fine motor skills like handwriting may also be affected, which can hinder communication.
Perception
Impaired sensory and visual perception means that those with ASD miss nonverbal cues, can be unaware of lies, and usually have difficulty seeing a situation from another person’s perspective.
TREATMENT
❯ Specialist interventions and therapies can assist with self-harming, hyperactivity, and sleep difficulties.
❯ Educational and behavioral programs can support the learning of social skills.
❯ Medication can help with associated symptoms— melatonin for sleep problems, SSRIs for depression, and methylphenidate for ADHD.
This neurodevelopmental disorder is diagnosed in children with behavioral symptoms (inattentiveness, hyperactivity, and impulsivity) that are inconsistent with their age.
What is it?
This is a condition that makes it difficult for a child to sit still and concentrate, and it is usually noticeable before the age of six. The effects of ADHD can persist into adolescence and adulthood. Adults may also be diagnosed with the preexisting condition, when persistent problems in higher education, employment, and relationships reveal it. However, the symptoms may not be as clear as they are in children (right). The level of hyperactivity decreases in adults with ADHD, but they struggle more with paying attention, impulsive behavior, and restlessness. The evidence for what causes ADHD is inconclusive, but it is thought to include a combination of factors. Genetics may play a part, which explains why it runs in families. Observations of brain scans also indicate differences in brain structure, and have identified unusual levels of the neurotransmitters dopamine and norepinephrine . Other possible risk factors include premature birth, low birthweight, and exposure to environmental hazards. The condition is more common in people with learning difficulties. Children with ADHD may also display signs of other conditions such as ASD , tic disorders or Tourette’s , depression , and sleep disorders . Surveys have shown that worldwide this condition affects more than twice as many boys as girls.
Identifying ADHD
A GP cannot officially diagnose ADHD, but if they suspect a child has the disorder they refer them for specialist assessment. The child’s patterns of hyperactivity, inattention, and impulsive behavior are observed over a six-month period before a treatment plan is prepared.
HYPERACTIVITY
❯ Difficulties sitting still The child cannot stay seated (or quiet) in situations where it is expected, such as the classroom.
❯ Constant fidgeting The child may twitch limbs, torso, and/or head, whether sitting or standing.
❯ Lack of volume control The child shouts and makes loud noises during normal everyday activities.
❯ Little or no sense of danger This may result in the child running and climbing in environments where these behaviors are neither safe nor appropriate.
INATTENTIVENESS
❯ Concentration difficulties This causes the child to make errors of judgment and mistakes. Along with constant movement, this can cause injury.
❯ Clumsiness The child is prone to dropping and breaking things.
❯ Easily distracted The child appears not to be listening and is unable to complete tasks.
❯ Poor organizational skills The child’s inability to concentrate has an impact on organizational abilities.
❯ Forgetfulness This results in the child losing things.
IMPULSIVITY
❯ Interrupting The child disrupts conversations regardless of the speaker or situation.
❯ Inability to take turns The child is unable to wait their turn in conversations and games.
❯ Excessive talking The child may change a topic often or focus obsessively on one.
❯ Acting without thinking The child is unable to wait in line or keep up with group pace.
MANAGING ADHD
There are a number of ways that parents can help their child to handle the condition.
❯ Create predictable routines to calm an ADHD sufferer. Schedule daily activities and keep them consistent. Make sure school timetables are clearly set, too.
❯ Set clear boundaries and make sure the child knows what is expected of them; praise positive behavior right away.
❯ Give clear instructions, either visual or verbal, whichever the child finds easier to follow.
❯ Use an incentive scheme, for example, have a star/points chart whereby a child can earn privileges for good behavior.
TREATMENT
❯ Behavioral therapies to help the child and their family manage day to day; psychoeducation for families and caregivers.
❯ Lifestyle management such as improving physical health and reducing stress to calm the child.
❯ Medication can calm (not cure) the person so that they are less impulsive and hyperactive. Stimulants increase dopamine levels and trigger the area of the brain involved in concentration.
“… an ADHD brain [is] like a browser with way too many open tabs.”
This disorder can result in children who do not bond with a caregiver in infancy. Unidentified reactive attachment disorder can be a precursor to lifelong impaired personal development.
What is it?
Attachment theory states that developing a strong emotional and physical bond with a primary caregiver is key to a child’s healthy personal development. Without such a bond a child can become increasingly detached, withdrawn, and distressed, and the physical symptoms relating to stress become obvious. Persistent disregard of a child’s basic physical needs, frequent changes of primary caregivers, and childhood abuse can disrupt a child’s ability to form social and emotional bonds. The child can develop markedly disturbed ways of relating socially, and may be unable to initiate or respond to social interactions. Disinhibited responses, such as a disregard for convention and impulsive behavior, used to be included in the assessment of this disorder, but these are now considered as a separate diagnosis of disinhibited social engagement disorder.
Long-term impact
Early neutral, negative, or even hostile environments are likely to have a long-term negative impact and affect a person right through to adulthood. An individual’s ability to make and maintain healthy relationships in later life is seriously compromised. Reactive attachment disorder can develop in early infancy, and the vulnerability it creates is associated with a wide range of disorders that affect both children and adults (below).
Associated disorders
Undiagnosed reactive attachment disorder is an underlying factor in a number of psychological problems that emerge in childhood or adulthood under clinical assessment.
TREATMENT
❯ Cognitive and behavioral therapies including cognitive behavioral therapy to examine habitual appraisals, dialectical behavior therapy to help severely affected adults, family therapy to promote good communication, anxiety management, and positive behavior support.
This is a short-term, stress-related psychological disorder that can follow a significant life event. Typically, a person’s reaction is stronger, or more prolonged, than expected for the type of event.
What is it?
Any stressful event can trigger anxiety, difficulty sleeping, sadness, tension, and inability to focus. However, if an individual finds an event especially hard, their reaction can be stronger and persist for months. In a child, the disorder can follow family conflicts, problems at school, and hospitalization. The child may become withdrawn and/or disruptive, and complain of unexplained pain or illness. Adjustment disorder is not the same as PTSD or ASR because the stress trigger is not as severe. It normally resolves within months as a person learns how to adapt to a situation and/or the stressor is removed. There is no way to predict whether one person is more likely to develop adjustment disorder than another. It comes down to how they respond to an event and their personal history. A GP initially assesses whether an individual’s symptoms may be due to another condition, such as ASR, before referring them for a psychological assessment.
Causes and outcome
Some life events are known to lead to adjustment difficulties of varying severity. Examples are the death of a friend or family member, divorce or relationship breakdown, moving, illness or injury, financial worries, or job stress.
SYMPTOMS BEGIN WITHIN 3 MONTHS
The onset can be traced to an event and symptoms are more severe than expected. They include defiant, impulsive behavior; 3 MONTHS sleeplessness; crying; feeling sad and hopeless; anxiety; and muscle tension.
SYMPTOMS RESOLVE IN 6 MONTHS
With therapy and removal of the stressor, a person can learn to turn negative thoughts into healthy actions to change how they respond to stress.
TREATMENT
❯ Psychotherapies such as cognitive behavioral therapy and/or family or group therapies to help identify and respond to stressors.
❯ Antidepressants to lessen symptoms of depression, anxiety, and insomnia, along with a psychotherapy.
Also called acute stress disorder, ASR can appear quickly after an exceptional physical or mental stressor such as a bereavement, a road traffic incident, or an assault, but does not usually last long.
What is it?
Symptoms of ASR are anxiety and dissociative behavior following exposure to a traumatic and unexpected life event. The person may feel disconnected from themselves, have difficulty handling emotions, suffer mood swings, become depressed and anxious, and have panic attacks. They often experience difficulty sleeping, poor concentration, and recurrent dreams and flashbacks, and may avoid situations that trigger memories of the event. Some individuals have physiological symptoms such as raised heart rate, breathlessness, excessive sweating, headaches, chest pain, and nausea. ASR is described as acute because the symptoms come on fast, but do not usually last.Symptoms of ASR can begin within hours of the stress and are resolved within a month; if they last longer they may turn into PTSD (opposite). ASR may resolve without therapy. Talking things over with friends or relatives can help those with the disorder understand the event and put it into context. Individuals may benefit from psychotherapies, too.
HOW DOES ASR DIFFER FROM PTSD?
ASR and PTSD are similar, but the time frames are different. The symptoms of ASR occur within a month of an event and they usually resolve within the same month. The symptoms of PTSD may or may not develop within a month of the event or events. PTSD is not diagnosed unless the symptoms have been evident for more than three months. There is an overlap between what the symptoms are. However, in ASR symptoms involving feelings, such as dissociation, depression, and anxiety, predominate. With PTSD the symptoms relate to a prolonged or persistent response to the fight-orflight mechanism . There is a higher risk of ASR developing in a person who has had PTSD or mental health issues in the past, and ASR can lead to PTSD.
REGULAR MEDITATION can benefit the relationship that those with ASR have with uncomfortable mental experiences and calm the fight-orflight response.
TREATMENT
❯ Psychotherapies such as cognitive behavioral therapy to identify and reevaluate thoughts and behaviors that maintain anxiety and low mood.
❯ Lifestyle management including supportive listening and stressrelieving practices such as yoga or meditation.
❯ Beta-blockers and antidepressants to ease physical symptoms in combination with psychotherapy.
80% of people with ASR develop PTSD 6 months later
This is a severe anxiety disorder that may develop anytime after a person experiences or witnesses a terrifying or life-threatening event, or series of events, over which they have little or no control.
What is it?
PTSD is seen in people who have been in military combat or a serious incident, or suffered prolonged abuse or the unexpected injury or death of a family member. The event itself activates the fight-orflight reflex in the brain and body, putting the person on hyperalert to deal with the consequences of the trauma and protect them from a repeat of the episode. An individual with PTSD feels that the threat remains, so their heightened response is maintained, causing an array of unpleasant symptoms including panic attacks, involuntary flashbacks, nightmares, avoidance and emotional numbing, anger, jumpiness, insomnia, and difficulty concentrating. These symptoms usually develop within a month of the event (but may not appear for months or years) and last for more than three months. PTSD can lead to other mental health problems, and excessive alcohol and drug use is common. Watchful waiting is advisable at first to see if the symptoms subside within three months as treatment too early can exacerbate PTSD.
Brain changes
PTSD is a survival reaction. The symptoms result from an aim to help survive further traumatic experiences, and include raised levels of stress hormones and other changes in the brain.
HIPPOCAMPUS PTSD increases stress hormones, which reduce activity in the hippocampus and make it less effective in memory consolidation. Both the body and mind remain hyperalert because the decision-making ability is reduced.
PREFRONTAL CORTEX Trauma affects the function of the prefrontal cortex, changing behaviors, personality, and complex cognitive functions such as planning and decision-making.
HYPOTHALAMUS In PTSD, the hypothalamus sends signals to the adrenal glands (on the kidneys) to release the hormone adrenaline into the bloodstream and increase the chances of survival.
AMYGDALA PTSD increases the function of the amygdala, activating the fight-orflight response and increasing sensory awareness.
TREATMENT
❯ Trauma-focused therapy such as cognitive behavioral therapy or eye movement desensitization and reprocessing (p.136) to help reduce the sense of current threat by working on memory of the event.
❯ Compassion-focused therapy to self-soothe from shame-based thoughts and images. Group therapy for vulnerable groups such as war veterans.
Previously known as hypochondria, this condition involves a person worrying excessively about becoming seriously ill, even if thorough medical examinations reveal nothing.
What is it?
Hypochondria is considered to be two separate conditions: illness anxiety disorder if there are no symptoms or they are mild, or somatic symptom disorder (pp.108− 109) if there are major physical symptoms causing emotional stress. People with illness anxiety disorder become excessively preoccupied with their health. Some have exaggerated feelings about an existing condition (about 20 percent do have heart, respiratory, gastrointestinal, or neurological problems). Others experience unexplained symptoms. They convince themselves that these symptoms indicate a serious illness that has been missed by medical teams. Illness anxiety is a long-term condition that fluctuates in severity and may worsen with age or stress. It can be triggered by a major life event.Someone who is anxious or depressed is more prone to the disorder. Assessment and treatment focus on stopping avoidance and reassurance behaviors (below), reevaluating health beliefs, and increasing the person’s tolerance of uncertainties.
Endless checks
Disbelief in medical opinion reaffirms the person’s anxiety and results in extra focus on the body part or illness, which causes panic and physical symptoms. Safety behaviors, such as avoiding situations for fear of exposure to disease, and reassurance from others provide brief respite.
TREATMENT
❯ Behavioral therapies such as attention training to keep from overattending to body sensations and help reevaluate beliefs.
Also known as excoriation and trichotillomania respectively, these are impulse-control disorders in which a person has recurrent, irresistible urges to pick at their skin or pull out their body hair.
What are they?
The expressed aim of skin pickers or hair pullers is to achieve perfect hair or skin, but the reverse is the result. Both behaviors can cause physical damage. A person with trichotillomania may pull hair from their scalp and/ or other parts of their body such as eyebrows, eyelashes, and legs (and sometimes also from pets), which can result in noticeable hair loss. They may also swallow the hair, which can cause vomiting, stomach pain, and bleeding that can lead to anemia. Skin picking can result in scabs, abrasions, and lesions that may become infected. Both of these conditions can also be associated with OCD . Skin picking and hair pulling often begin as a reaction to an immediate stress or may be a response to a traumatic experience or abuse. The behavior can be learned from other members of the family with similar habits or develop by chance and become associated with stress relief, which is a powerful behavioral reinforcement. Females are more likely to be affected, and symptoms often start in girls aged 11–13 years. Hair pulling or skin picking can cause significant impairment or disruption in daily life for affected individuals. They may avoid routine activities or work, have difficulty concentrating, become socially isolated, and suffer financial strain.
Repetitive behavior
Habits associated with these disorders often begin as a response to stress or anxiety but become addictive—the more that a person pulls or picks, the greater their urge to do it, in spite of the various negative consequences.
TREATMENT
❯ Behavioral therapies to promote healthy stress management. Habit reversal training, combining awareness with alternative behavior, and stimulus control using a different activity while an urge dissipates.
In this condition a person has a distorted perception of how they look. The individual typically spends an excessive amount of time worrying about their appearance and how others view them.
What is it?
BDD is an anxiety disorder that can have a huge impact on daily life. An individual with BDD worries obsessively about how they look. They often focus on a specific aspect of their body, for example, viewing a barely visible scar as a major flaw or seeing their nose as abnormal, and are convinced that others view the “flaw” in the same way. The person may spend a great deal of time concealing an aspect of their appearance, seeking medical treatment for the part of the body believed to be defective, and/or diet or exercise excessively. BDD affects about 1 in every 50 people in the US, can occur in all age groups, and is seen in males and females in equal numbers. It is more common in people with a history of depression or social anxiety disorder ,and it often occurs alongside OCD (pp.56–57) or generalized anxiety disorder (GAD, ). BDD may be due to brain chemistry or genetics, and past experiences may play a role in triggering its development. In assessment, the doctor asks the person about their symptoms and how they affect them and may refer them to a mental health specialist for further treatment.
Breaking the cycle
LOW MOOD The perceived constant social threat leads to chronic anxiety and depression.
EFFORTS TO CHANGE APPEARANCESafety behaviors or social avoidance prevail. The person may apply excessive makeup or use clothing to conceal the perceived defective attribute; seek cosmetic surgery; use extreme diet and exercise to change body shape; and avoid social situations, thus increasing feelings of isolation.
TRIGGER Seeing their reflection, misinterpreting body language, or someone’s passing comment can start the cycle.
AUTOMATIC THOUGHTS Negative thoughts dominate, for example, “I am defective and defective people are worthless, so I am worthless.”
TREATMENT
❯ Cognitive behavioral therapy to identify self-appraisal related to the problem body part and weaken the beliefs that maintain it.
❯ Antidepressants and antianxiety medication alongside therapy.
Also known as compulsive hoarding, this disorder is characterized by the excessive acquisition of, and/or the inability or unwillingness to dispose of, large quantities of objects.
What is it?
Hoarding disorder may begin as a way of coping with a stressful life event. The individual with does not discard worn-out possessions, for fear either of needing them again or of something bad happening to other people if they get rid of anything. They store sentimental items because they believe that discarding them will keep emotional needs from being met. The individual continues to accumulate items even when space is running out. Hoarding can be hard to treat because the person does not see it as a problem and experiences such overwhelming discomfort at reducing the clutter that they avoid any attempt to do so. Alternatively, the person may be aware of the problem but too ashamed to seek help or advice. Hoarding may be part of other disorders such as OCD , severe depression , or psychotic disorders . In assessment, the doctor questions the person about their feelings on acquiring objects and their overestimation of responsibility for causing harm by discarding items.
Living with hoarding
A person with hoarding disorder may let junk mail, bills, receipts, and heaps of paper pile up. The resulting clutter can pose a health and safety risk and makes it hard to move from room to room, which is distressing for the individual and affects their, and their family’s, quality of life. This may lead to isolation and impaired or difficult relationships with other people.
TREATMENT
❯ Cognitive behavioral therapy to examine and weaken the thoughts that maintain the hoarding behavior and allow adaptive or flexible alternatives to emerge.
❯ Lifestyle management at home to motivate reducing clutter for health and safety reasons.
❯ Antidepressants to decrease the associated anxiety and depression.
This is a debilitating anxiety-related condition characterized by intrusive and unwelcome obsessive thoughts that are often followed by repetitive compulsions, impulses, or urges.
What is it?
OCD is often marked by thoughts that reflect an excessive sense of responsibility for keeping others safe and an overestimation of the perceived threat an intrusive thought signifies. OCD is cyclical (below) and often starts with an obsessive thought, which the person focuses on, in turn raising anxiety levels. Checking everything is in order and following rituals can provide relief, but the distressing thought returns.The obsessive thoughts and compulsions are timeconsuming, and individuals may struggle to function day to day or have a disrupted social or family life. The disorder may be triggered by an event in the person’s history that they felt highly responsible for. Family history, differences in the brain, and personality traits also play a part. An examination of thoughts, feelings, and behavior patterns determines OCD, but its similarity to other anxiety disorders can make diagnosis difficult. With pure OCD, a person has intrusive and disturbing thoughts about harming people, but rather than performing observable compulsions, their compulsions take place in the mind.
OBSESSIONS (THOUGHTS)
Fear of causing harm Excessive attention paid to thoughts about actions that could cause harm.
Intrusive thoughts Obsessive, repetitive, and even disturbing thoughts about causing harm.
Fear of contamination Thinking that something is dirty or germ-ridden and will cause illness or death to the person or someone else.
Fear related to order or symmetry Concern that harm could result unless tasks are done in a specific order.
COMPULSIONS (BEHAVIORS)
Rituals Following rituals such as counting or tapping to prevent harm and provide relief from the cycle of fear.
Constant checking Examining household appliances, lights, taps, locks, windows (to counter fear of causing harm by fire), driving routes (fear of having run a person over), or people (fear of upsetting someone).
Correcting thoughts Trying to neutralize thoughts to prevent disasters.
Reassurance Repeatedly asking others to confirm everything is OK.
FOLLOWING RITUALS and constant checking that everything is in order and safe are the main features of OCD.
TREATMENT
❯ Cognitive behavioral therapy involving exposure to triggers and learning how to control responses.
❯ Anti-anxiety medication and/or antidepressants to help relieve symptoms of depression and anxiety.
❯ Specialist residential treatment in addition to therapy and medication for extremely severe cases of OCD.
“An average person can have four thousand thoughts a day, and not all of them are useful or rational.”
This is an anxiety disorder in which people are unable to talk in certain social situations, but are able to speak at other times. It is usually first recognized between the ages of three and eight years.
What is it?
Selective mutism is associated with anxiety, and children who are affected by it struggle with excessive fears and worries. They are generally able to speak freely where they feel comfortable but are unable to talk in specific situations, when they do not engage, go still, or have a frozen facial expression when expected to talk. This inability to speak is not the result of a conscious decision or a refusal. The mutism can be triggered by a stressful experience, or it can stem from a speech or language disorder, or hearing problem, that makes social situations involving communication particularly stressful. Whatever the cause, everyday activities are difficult, as are relationships within the family or school. Treating the condition can prevent it from persisting into adulthood—the younger the child is when diagnosed, the easier it is to treat. If symptoms persist for more than a month, the child should be seen by a GP, who can refer them for speech and language therapy. A specialist asks whether there is a history of anxiety disorders, a likely stressor, or a hearing problem. Treatment depends on how long the child has had the condition, the presence of learning difficulties or anxieties, and the support that is available.
State of fear
TREATMENT
❯ Cognitive behavioral therapy using positive and negative reinforcements to build speech and language skills; graded exposure to specific situations to reduce anxiety, removing pressure on the child to speak.
❯ Psychoeducation can provide information and support for parents and caregivers, relieve general anxiety, and reduce chances of the disorder persisting
“It is a child suffering in silence.”
Dr. Elisa Shipon-Blum, American president of Selective Mutism Anxiety Research and Treatment Center
This anxiety disorder can develop in children whose natural concern about being separated from their parent, primary caregiver, or home persists beyond the age of two years.
What is it?
Separation anxiety is a normal adaptive reaction that helps to keep babies and toddlers safe while they attain competence to cope with their environment. However, it can be a problem if it persists for more than four weeks and interferes with age-appropriate behavior. The child becomes distressed when they need to leave a primary caregiver and fears that harm will come to that person. Situations such as school and social occasions can also be a trigger. Affected children may experience panic attacks, disturbed sleep, clinginess, and inconsolable crying. They may complain of physical problems such as stomachache, headache, or just feeling unwell for no apparent reason. Older children may anticipate feelings of panic and struggle to travel independently. Separation is the most common VIVID FEARS The child worries excessively about being detached from their primary caregiver—even if only in a separate room. anxiety disorder in children under 12 years old. It can also affect older children, and it may be diagnosed in adulthood. The disorder can develop after a major stressor such as the loss of a loved one or pet, moving, changing schools, or parents’ divorce. Overprotective or intrusive parenting can contribute. Separation anxiety is very treatable with behavioral therapies that include building planned separations into times of the day when the person is feeling least vulnerable.
Being alone
Vivid fear
UNWANTED BURDEN
TREATMENT
❯ Cognitive behavioral therapy for anxiety management; assertiveness training for older children and adults.
❯ Parent training and support to promote and reinforce short periods of separation that are then extended gradually.
❯ Anti-anxiety medication and antidepressants for older individuals, in combination with environmental and psychological interventions.
Individuals with this condition experience an overwhelming fear of being judged or of doing something embarrassing in social situations. The disorder can cause disabling self-consciousness.
What is it?
An individual with social anxiety disorder (also called social phobia) experiences excessive nerves or dread of social situations. They may be anxious only in specific circumstances, such as speaking or performing in public, or experience distress in all social situations. The person tends to be extremely self-conscious and worries about others evaluating them negatively. They dwell on past social incidents, obsessing about how they might have come across. Social anxiety causes the person to overplan and rehearse for anticipated situations, which may lead to odd or awkward behavior. Individuals may then gather evidence to support their fears, because difficult situations often arise as a result of the person’s anxiety or over-rehearsal. This disorder leads to isolation and depression and can seriously affect social relationships. It can also have a negative impact on performance at work or school.
SYMPTOMS BEFORE SOCIAL INTERACTION The individual may prepare and rehearse excessively in advance, planning topics of conversation or how to present themselves in a specific way.
DURING INTERACTION Physical symptoms such as trembling, rapid breathing, racing heart, sweating, or blushing occur as the body’s “fight or flight” system is activated. In extreme cases, the person may experience a panic attack.
AFTER INTERACTION The person conducts a detailed, negative, and self-critical appraisal of the social situation, dissecting conversations and body language and giving them a negative slant.
TREATMENT
❯ Cognitive behavioral therapy to recognize and change negative thought patterns and behaviors.
❯ Group therapy for the opportunity to share problems and practice social behavior.
❯ Self-help including affirmations, rehearsing before social events, and using video feedback to disprove negative assumptions.
People with this disorder experience continual unrestrained and uncontrollable worry (even when no danger is present), to the extent that day-to-day activity and functioning can become impaired.
What is it?
An individual with GAD worries excessively about a wide range of issues and situations. Symptoms include “threat” reactions such as heart palpitations, trembling, sweating, irritability, restlessness, and headaches. GAD can also cause insomnia and difficulty in concentrating, making decisions, or dealing with uncertainty. The person may become obsessed with perfectionism, or with planning and controlling events. The physical and psychological symptoms can have a debilitating effect on social interactions, work, and everyday activities, leading to lowered confidence and isolation. Worries may revolve around family or social matters, work, health, school, or specific events. A person with GAD experiences feelings of anxiety most days, and as soon as they Social fears resolve one worry another appears. They overestimate the likelihood of bad or dangerous things happening and resolve one worry another appears. They overestimate the likelihood of bad or dangerous things happening and predict the worst possible outcome. The individual may even report positive beliefs about the helpfulness of worry, such as “Worrying makes it less likely that bad things will happen.” Long-term or habitual avoidance of fearful situations or places compounds the disorder, because the individual never gathers evidence that their fears are unfounded, thus maintaining the worry.
Balancing worries
Anxiety becomes a problem when a person is weighed down with worries for the majority of days in a six-month period or longer.
Social fears
Health or money worries
Anticipation of dangers and disasters
Perfectionism
TREATMENT
❯ Cognitive behavioral therapy to identify triggers, negative thoughts, habitual avoidance, and safety behaviors.
❯ Behavioral therapy to identify new behavioral goals, with achievable steps.
❯ Group therapy with assertiveness training and building self-esteem to help counteract unhelpful beliefs and unfounded fears.
An irrational fear of becoming trapped in a confined space or even the anticipation of such a situation, claustrophobia is a complex phobia that can cause extreme anxiety and panic attacks.
FEAR OF CONFINED SPACES is normal if the threat is genuine, but a person with claustrophobia has an irrational fear regardless of actual danger.
What is it?
For a person with claustrophobia, being confined induces physical symptoms similar to those of agoraphobia (opposite). The fear also increases negative thoughts of running out of oxygen or suffering a heart attack with no chance of escape. Many individuals also experience feelings of dread and fear of fainting or losing control. Claustrophobia may be caused by conditioning following a stressful situation that occurred in a small space. This might be traced back to childhood, when, for example, an individual was confined in a tiny room or was bullied or abused. The condition can also be triggered by unpleasant experiences at any stage of life, such as turbulence on a flight or being trapped in an elevator. The individual fears a repeat of being confined and overimagines what could happen in a small space. As a result they plan their daily activities carefully to minimize the likelihood of “becoming trapped.” Sometimes claustrophobia is observed in other family members, which suggests a genetic vulnerability to the disorder and/or a learned associated response.
TREATMENT
❯ Cognitive behavioral therapy to reevaluate negative thoughts through exposure to the feared situation in small steps so the individual realizes that the worst fear does not occur.
❯ Anxiety management to cope with anxiety and panic by using breathing techniques, muscle relaxation, and visualization of positive outcomes.
❯ Anti-anxiety medication or antidepressants prescribed in extreme cases.
This is an anxiety disorder characterized by a fear of being trapped in any situation in which escape is difficult or rescue is unavailable if things go wrong.
What is it?
Agoraphobia is a complex phobia that is not, as many think, simply a fear of open spaces. The individual dreads being trapped, and avoids whatever triggers the terror of being unable to escape. The result can be a fear of traveling on public transport, being in an enclosed space or a crowd, going shopping or to health appointments, or leaving the house. The associated panic attack brought on by such an experience is accompanied by negative thoughts—for example, the person may think that as well as being trapped they are going to look ridiculous, because they are out of control in public. The symptoms, or fear of them, are disruptive and result in avoidance behaviors that make leading a normal life hard. Agoraphobia can develop if an individual has a panic attack, then worries excessively about a repeat experience. In the UK, one-third of those who have panic attacks go on to develop agoraphobia. Biological and psychological factors are the probable cause. Experiencing or witnessing a traumatic event, mental illness, or an unhappy relationship may play a part. Treatment can help—about one-third are cured and 50 percent find that symptoms improve. A GP first excludes other conditions that may be causing the symptoms.
Types of symptoms
SYMPTOMS
PHYSICAL Rapid heart and breathing rate, chest pain, dizziness, shaking, feeling nauseous, and breathing problems.
BEHAVIORAL Excessive planning to avoid crowds, lines, and public transport, or not going out at all or only with a trusted person.
COGNITIVE Predictions of shaming by others, overthinking potential disasters, catastrophic thoughts of being trapped or injured, and feeling out of control.
TREATMENT
❯ Intensive psychotherapy such as cognitive behavioral therapy to explore the thoughts that maintain the phobia; behavioral experiments to gather evidence that defuses strongly held beliefs.BEHAVIORAL Excessive planning to avoid crowds, lines, and public transport, or not going out at all or only with a trusted person.
❯ Self-help groups using safe visual material to work on exposure to the feared situation; teaching how to manage a panic attack by breathing slowly and deeply.
❯ Lifestyle management such as exercise and a healthy diet.
“Nothing diminishes anxiety faster than action.”
Walter Inglis Anderson, American painter, writer, and naturalist
A phobia is a type of anxiety disorder. Specific phobias manifest themselves when a person anticipates contact with, or is exposed to, the object, situation, or event they fear.
What are they?
Specific, simple phobias (as opposed to the complex ones, agoraphobia and claustrophobia, pp.50–51) are the most common psychological disorders in children and adults. A phobia is much more than fear and arises when a person develops an exaggerated or unrealistic sense of danger about a situation or an object. The fear may not make any sense, but the individual feels powerless to stop it. Anticipated or actual exposure (even to an image) can cause extreme anxiety or a panic attack. Symptoms include rapid heart rate, breathing difficulties, and a feeling of being out of control. A combination of genetics; brain chemistry; and other biological, psychological, and environmental factors can give rise to a phobia. It can often be traced back to a frightening event or stressful situation a person either witnessed or was involved in during early childhood. A child can also “learn” a phobia through seeing other family members demonstrate phobic behavior. Specific phobias often develop during childhood or adolescence and may become less severe with age. They can also be associated with other psychological conditions such as depression , obsessive compulsive disorder , and post-traumatic stress disorder .
How are they diagnosed?
Many affected individuals are fully aware of their phobia, so a formal diagnosis is not necessary and they do not need treatment—avoiding the object of their fear is enough to control the problem. However, in some people habitual avoidance of a feared object can also maintain or worsen the phobia, and seriously impact aspects of their lives. A GP can refer them to a specialist with expertise in behavioral therapy.
Types of specific phobia
There is a wide variety of objects or situations that can trigger a phobia. Specific, so-called “simple,” phobias fall into five groups: blood-injectioninjury, natural environment, situational, animal, and “other” types. With the exception of the first type, specific phobias are two to three times more common in females than males.
ANIMAL This group of phobias includes insects, snakes, mice, cats, dogs, and birds, among other animals. It could be rooted in a genetic predisposition for survival from animals that were a threat to human ancestors.
SNAKES
SPIDERS
RATS
BLOOD-INJECTION-INJURY
A unique group of phobias in which the sight of blood or needles causes a vasovagal reaction—a reflex action that slows down the heart rate, reducing blood flow to the brain—that can result in fainting. Unlike all other phobias, this is as common in males as it is in females.
NEEDLES
BLOOD
SITUATIONAL
These are a group of phobias of being in a specific situation, which can range from visiting the dentist’s office to stepping into an old elevator, flying, driving over a bridge or through a tunnel, or getting into a car.
FLYING
BRIDGES
NATURAL ENVIRONMENT
A person with a phobia from this group has an irrational fear of a natural event, which they often associate with imagery of potentially catastrophic outcomes. Examples of this type of phobia include storms; deep water; germs; and fear of heights, such as being near a cliff edge.
WATER
HEIGHTS
LIGHTNING
SPECIFIC PHOBIAS are very treatable with gradual, guided exposure to the feared object or situation.
OTHER PHOBIAS
Thousands of people are tormented by an array of phobias, including fear of vomiting; a specific color, for example, anything that is yellow or red (including foodstuffs); the number 13; the sight of a belly button or toes; sudden loud noises; costumed characters, such as clowns; trees; or contact with cut flowers.
TREES
CLOWNS
TREATMENT
❯ Cognitive behavioral therapy to overcome a phobia using a system of graded steps to work toward the goal of confronting the feared object or situation without fear; anxiety management techniques to master each step.
❯ Mindfulness to raise tolerance of anxiety and of thoughts or images associated with the distress.
❯ Anti-anxiety medication or antidepressants alongside therapy if the phobia is impairing day-to-day living.
8.7% of adult Americans are affected by a specific phobia
Panic attacks are an exaggerated reaction to the body’s normal response to fear or excitement. With panic disorder, a person regularly experiences such attacks for no obvious reason.
What is it?
The normal reaction to fear or excitement causes the body to produce the hormone adrenaline to prepare for “fight or flight” from the source of fear. If a person has a panic attack, apparently normal thoughts or images trigger the brain’s fight-or-flight center, resulting in adrenaline racing around the body causing symptoms such as sweating, increased heart rate, and hyperventilation. Attacks last about 20 minutes and can be very uncomfortable. The individual may misinterpret these symptoms, saying they feel as if they are having a heart attack or even dying. The fear can further activate the brain’s threat center so more adrenaline is produced, worsening symptoms. Individuals who have recurring panic attacks can fear the next one so much that they live in a constant state of “fear of fear.” Attacks may, for example, be set off by fear of being in a crowd or a small space,but often they are triggered by internal sensations that have nothing to do with the outside world. As a result, everyday tasks can become difficult and social situations daunting. Those with panic disorder may avoid certain places or activities, so the problem persists because the person can never “disconfirm” their fear.
What are the causes?
One in 10 people suffer from occasional panic attacks; panic disorder is less common. Traumatic life experiences, such as a bereavement, can trigger the disorder. Having a close family member with panic disorder is thought to increase the risk of developing it. Environmental conditions such as high carbon dioxide levels may also cause attacks. Some illnesses, for example an overactive thyroid, can produce symptoms similar to panic disorder, and a doctor will rule out such illnesses before making a diagnosis.
2% of people are affected by panic disorder
The panic cycle
Constant cycle of anxiety and fear
A person perceives a threat and starts to panic. The physical symptoms develop, worsening the anxiety and therefore the symptoms, which in turn increase the likelihood of a repeat attack.
SYMPTOMS OF A PANIC ATTACK
The symptoms result from the action of the autonomic nervous system—the part not under conscious control
Increased heart rate Adrenaline causes the heart to pump faster to move blood containing oxygen to where it is needed. This can result in chest pains.
Feeling faint Breathing is faster and shallower to increase The panic cycle oxygen, causing hyperventilation and lightheadedness.
Sweating and pallor Sweating increases to cool the body. The person may also become pale as blood is diverted to where it is needed most.
Choking sensation Faster breathing feels like choking—oxygen level rises but not enough carbon dioxide is exhaled.
Dilated pupils The pupil (black part of the eye) becomes dilated to let in more light, making it easier to see to escape.
Slowed digestion As digestion is not crucial for “flight,” it slows. The sphincters (valves) relax, which makes the sufferer feel nauseous.
Dry mouth The mouth can feel very dry as body fluids are concentrated in the parts of the body where they are most needed.
TREATMENT
❯ Cognitive behavioral therapy to identify triggers, prevent avoidance behavior, and learn to disprove feared outcomes. ❯ Support groups to meet others with the disorder and get advice. ❯ Selective serotonin reuptake inhibitors (SSRIs) .
SAD is a form of seasonal depression linked to changing levels of light that typically starts in fall as the days shorten. It is also known as “winter depression” or “hibernation state.”
What is it?
The nature and severity of SAD vary from person to person, and for some it can have a significant impact on their day-to-day life. Typically the symptoms come and go with the seasons, and always begin at the same time of year, often in the fall. Symptoms include low mood, a loss of interest in everyday activities, irritability, despair, guilt, and feelings of worthlessness. People with SAD lack energy, feel sleepy during the day, sleep for longer than normal at night, and find it hard to get up in the morning. As many as one in three people are affected. SAD’s seasonal nature can make diagnosis difficult. Psychological assessment looks at a person’s mood, lifestyle, diet, seasonal behavior, thought changes, and family history.
Seasonal cause and effect
Sunlight level affects a part of the brain called the hypothalamus by altering the production of two chemicals: melatonin (which controls sleep) and serotonin (which changes mood).
Winter pattern
❯ Melatonin increases so person is tired and wants to sleep. ❯ Serotonin productiondrops, causing person to feel low. ❯ Desire to stay in bed and sleep can lead to reduced social contact. ❯ Craving carbohydrates can cause overeating and weight gain. ❯ Constant daytime fatigue affects work and family life.
Secretion of melatonin by the pineal gland is triggered by darkness/ inhibited by light and controlled by the hypothalamus.
Summer pattern
❯ Melatonin drops so person has more energy.
❯ Serotonin production increases, improving mood and outlook.
❯ Sleep is good, but not excessive, so person has more energy.
❯ Diet improves as cravings subside.
❯ Improved energy results in increased activity and more social contact.
DMDD is a childhood disorder characterized by almost constant anger and irritability combined with regular and severe temper tantrums.
What is it?
DMDD is a recently identified disorder that children with a history of chronic irritability and serious temper outbursts are now recognized as having. The child is sad, bad-tempered, and/or angry almost every day. The outbursts are grossly out of proportion with the situation at hand, occur several times every week, and happen in more than one place (at home, at school, and/or with peers). Strained interactions that occur only between a child and their parents, or a child and their teacher, do not indicate DMDD.
How is it diagnosed?
For a diagnosis of DMDD, the symptoms must be evident consistently for more than a year, and interfere with a child’s ability to function at home and at school. One cause can be that the child misinterprets other people’s expressions, in which case training in facial-expression-recognition can be offered. Diagnosed children are generally under the age of 10, but not younger than 6 or older than 18. One to 3 percent of children under the age of 10 have symptoms.Children with DMDD were once identified as having pediatric bipolar disorder, but they do not present with the episodic mania or hypomania of that disorder. They are unlikely to develop bipolar, but are at a higher risk of depression and anxiety as adults.
Disruptive behavior
Children with DMDD regularly have severe temper tantrums, inconsistent with their developmental stage, three or more times a week in at least two different settings.
TREATMENT
❯ Psychotherapy for both child and family to explore emotions and develop mood management techniques.
❯ Lifestyle management including positive behavior support to establish better communication and minimize outburst triggers.
❯ Antidepressants or antipsychotics to support psychotherapy.
Occurring at any time during pregnancy and up to a year after giving birth, perinatal mental illnesses include PPD (postpartum depression), sometimes called postnatal depression, and postpartum psychosis.
What is it?
Feeling tearful or irritable just after giving birth is so common it is dubbed the “baby blues,” but these feelings last for only a couple of weeks. What sets PPD apart from baby blues is the length of time it lasts. It is a longer-term moderate to severe depression that can develop in new mothers (and occasionally fathers) at any time in the year after birth. Symptoms include constant low mood or mood swings, low energy levels, difficulty bonding with the baby, and frightening thoughts. The individual may cry easily and profusely and feel acutely fatigued yet have sleep problems. Feelings of shame and inadequacy, worthlessness, and fear of failure as a parent are common. In severe cases, panic attacks, self-harm, and thoughts of suicide occur. However, most individuals make a full recovery. Untreated, PPD may last for many months or longer. PPD can develop suddenly or slowly, and is usually caused by hormone and lifestyle changes and fatigue. It is not clear why some people develop PPD, but risk factors appear to include difficult childhood experiences, low self-esteem, a lack of support, and stressful living conditions.
How is it diagnosed?
To determine whether an individual has PPD, a doctor, midwife, or health professional assesses symptoms using an efficient and reliable screening questionnaire such as the Edinburgh Postnatal Depression Scale, which rates mood and activity levels over the previous seven days. Other assessment scales are used to assess mental well-being and functioning. Good clinical judgment is needed when interpreting the results of these questionnaires as new parents are likely to be less active simply as a result of their new responsibilities.
POSTPARTUM PSYCHOSIS
An extremely serious condition, postpartum psychosis (also known as puerperal psychosis) affects 1–2 women per 1,000 births. It usually occurs in the first few weeks after delivery, but may begin up to six months after birth. Symptoms often develop rapidly and include confusion, high mood, racing thoughts, disorientation, paranoia, hallucinations, delusions, and sleep disturbance. The individual may also have obsessive thoughts about the baby, and attempt to self-harm or harm the baby. Immediate treatment is needed because of the potentially life-threatening thoughts and behaviors associated with the disorder. Treatment comprises hospitalization (usually in a highly monitored mother-and-baby treatment unit), medication (antidepressants and antipsychotics), and psychotherapy.
TREATMENT
❯ Cognitive and behavioral therapies in a group, one-on-one, or as guided self-help; one-on-one counseling
❯ Lifestyle management, such as talking to partner, friends, and family; resting; regular exercise; and eating healthily and regularly.
❯ Antidepressants alone or with psychotherapy.
Range of symptoms
The symptoms of postpartum depression are similar to those of anxiety and general depression. Symptoms can make it difficult to complete day-to-day activities and routines, and can affect an individual’s relationship with their baby, partner, family, and friends.
This condition is characterized by extreme swings—highs (mania) and lows (depression)—in a person’s energy and activity levels, which is why it was originally called manic depression.
What is it?
There are four types of bipolar disorder: bipolar 1 is severe mania lasting for more than a week (the person may need hospitalization); bipolar 2 causes swings between a less severe mania and low mood; cyclothymia features longer-term hypomanic and depressive episodes lasting for up to two years; and unspecified bipolar disorder is a mixture of the three types. During a mood swing an individual can undergo extreme personality changes, which puts social and personal relationships under severe strain. The main cause of bipolar is commonly believed to be an imbalance of the chemicals involved in brain function. Known as neurotransmitters, these chemicals include norepinephrine, serotonin, and dopamine, and relay signals between nerve cells . Genetics also play a role: bipolar disorder runs in families, and it can develop at any age. It is thought that 2 in every 100 people have an episode at some stage; some have only a couple in their lifetime, whereas others have many. Episodes may be triggered by stress; illness; or hardships in everyday life, such as relationship difficulties or problems with money or work.
How is it diagnosed?
The affected person is assessed by a psychiatrist or clinical psychologist, who asks about the symptoms and when they first occurred. Signals leading up to an episode are explored, too. The doctor also looks to eliminate other conditions that can cause mood swings. The individual is usually treated with medication and lifestyle management techniques.
Patterns of depression and mania
There are distinct phases to the mood swings of bipolar disorder. The extent and timescale of fluctuations and the way moods manifest themselves and affect personality can vary widely.
BALANCED/NORMAL MOOD This is a state between episodes in which the person copes with regular daily routines and can plan and predict the consequences of day-to-day actions.
DEPRESSION The person cannot experience pleasure; has difficulty sleeping; has no appetite; may be delusional; or has hallucinations and disturbed, even suicidal, thoughts.
HYPOMANIA In this form of mania, lasting a few days, an individual can be highly productive and function well. It can precede full mania.
MILD DEPRESSION This is characterized by sadness, low energy, and an inability to concentrate. A person may lack motivation and lose interest in everyday activities.
MANIA This severe form may last a week or more. Symptoms include hyperactivity; rapid, uninterruptable, and loud speech; risktaking; lack of sleep; and inflated self-image.
MIXED STATE The person suffers from mania at the same time as depression. The individual may, for example, be hyperactive and have depressive symptoms at the same time.
TREATMENT
❯ Cognitive behavioral therapy
❯ Lifestyle management including regular exercise; better diet; sleep routines, which may improve mood regulation; and use of diaries and daily awareness methods, which may help the individual to recognize signs of mood changes.
❯ Mood stabilizers taken long term to minimize likelihood of mood swings; dosage often adjusted during episodes of hypomania, mania, or depression.
“[Bipolar] is a challenge, but it can set you up to be able to do almost anything.”
This is a common condition that may be diagnosed when a person has been feeling down and worried—and has lost pleasure in daily activities—for more than two weeks.
What is it?
The symptoms of depression can include continuous low mood or sadness, having low self-esteem, feeling hopeless and helpless, being tearful, feeling guilt-ridden, and being irritable and intolerant of others.A person with depression is unmotivated and uninterested, finds it difficult to make decisions, and takes no enjoyment from life. As a result, the individual may avoid the social events that they usually enjoy, thus missing out on social interaction, which can cause a vicious circle which sees them spiraling further downward. Depression can make it difficult for a person to concentrate and remember things. In extreme cases the sense of hopelessness may lead to thoughts of self-harm or even suicide.
Internal and external causes
A wide range of biological, social, and environmental factors can cause depression. External causes predominantly encompass life events that can have a negative impact on a person, and often act in combination with internal causes—those within an individual—to trigger depression.
Many internal and external factors (left), such as childhood experiences and life events, physical illness, or injury, can cause depression. It can be mild, moderate, or severe and is extremely common—according to the World Health Organization, more than 350 million people suffer from it globally.
EXTERNAL CAUSES
Money, or the lack of it, and the stress caused by financial concerns and worries about debt.
Stress when a person cannot cope with the demands placed on them.
Job/unemployment impacting status and self-esteem, perception of a positive future, and ability to engage socially.
Bereavement following the death of a family member, friend, or pet.
Alcohol and drugs due to the physiological, social, and economic consequences of addiction.
Bullying among children and adults, whether physical or verbal, face to face or online.
Pregnancy and birth and the overwhelming prospect of parenthood for new mothers.
Relationship problems leading to depression in the longer term.
Loneliness as a result of health or disability, especially in the elderly.
INTERNAL CAUSES
Personality traits, such as neuroticism and pessimism.
Childhood experiences, especially if the person felt out of control and helpless at the time.
Family history, if a parent or sibling has had depression.
Long-term health problems, such as heart lung or kidney disease; diabetes; and asthma.
How is it diagnosed?
A doctor can diagnose by asking the person questions about their particular symptoms. One objective is to find out how long the symptoms have been going on. The doctor may also suggest blood tests to rule out any other illness that may cause the symptoms of depression. Subsequent treatment depends on the severity of the depression, but the main option is to undergo psychotherapy. Antidepressants may be offered to help the person cope with everyday life. For mild to moderate depression, exercise can be helpful. In severe cases, hospital admission or medication for psychotic symptoms may be needed.
FEELINGS OF LONELINESS result from depression and cause a person to feel completely alone, helpless, and isolated.
TREATMENT
❯ Cognitive and behavioral therapies such as behavioral activation, cognitive behavioral therapy , compassion focused, acceptance and commitment , and cognitive therapies.
❯ Psychodynamic psychotherapy and counseling.
❯ Antidepressants on their own or alongside therapy.
“… depression is so insidious … it’s impossible to ever see the end.”
The medical diagnosis of a mental health condition is a complex process of matching an individual’s pattern of physical and psychological symptoms to behaviors associated with a disorder, or disorders. Some conditions, such as a learning disability or neuropsychological problems, are easily identified. Functional disorders that affect personality and conduct are more difficult, however, as they involve numerous biological, psychological, and social factors.
What are mental health disorders?
Mental health disorders are characterized by the presence of unusual or abnormal mood, thinking, and behaviors that cause an individual significant distress or impairment, and disrupt their ability to function. Impairment occurring as the result of common stressors such as bereavement would not be considered a disorder. Diverse social and cultural factors impacting behaviors might also rule out the presence of mental health problems.
CATEGORIES OF DISORDERS
❯ Mood disorders
❯ Anxiety disorders
❯ Obsessive compulsive and related disorders
❯ Trauma- and stress-related disorders
❯ Neurodevelopmental disorders
❯ Psychotic disorders
❯ Neurocognitive disorders
❯ Addictive and impulse-control disorders
❯ Dissociative disorders
❯ Eating disorders
❯ Communication disorders
❯ Sleep disorders
❯ Motor disorders
❯ Personality disorders
❯ Other
Disorders can be classified into diagnostic groups (above); the two main works used to identify, categorize, and organize them are the World Health Organization’s International Classification of Disease (ICD-10) and the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
Assessment of a mental health condition
Clinical diagnosis is made only after a careful assessment process that includes observation and interpretation of a person’s behaviors and discussion with them and, if relevant, their family, caregivers, and specialist professionals. Putting a name to a person’s distress can help them—and their support systems—gain a deeper understanding of their difficulties and how to manage them better, but it can also negatively shape a person’s outlook and contribute to self-fulfilling prophecies.
Physical examination
A GP will first eliminate physical illness that could be causing symptoms. Medical examination can also reveal intellectual disabilities or speech disorders due to physical abnormalities. Imaging techniques may be used to test for brain injury or dementia, and blood tests can reveal a genetic predisposition to certain disorders.
Clinical interview
If no physical illness is identified, an individual may be referred to a mental health specialist. They will ask the client about their life experiences, their family history, and recent experiences that relate to their problem. The conversation will also aim to uncover any predisposing factors, strengths, and vulnerabilities.
Psychological tests
Particular aspects of a person’s knowledge, skill, or personality will be evaluated through a series of tests and/or tasks, usually in the form of checklists or questionnaires standardized for use on very specific groups. For example, such tests may measure adaptive behaviors, beliefs about the self, or traits of personality disorders.
Behavioral assessment
A person’s behavior will also be observed and measured, normally in the situation where their difficulties occur, to gain an understanding of the factors that precipitate and/or maintain their symptoms. The person might also be asked to make their own observations by recording a mood diary or using a frequency counter.
1in4 36 37 people will be affected by mental or neurological disorders in their lifetime
PSYCHOLOGICAL DISORDERS The distressing symptoms of a psychological disorder often go hand in hand with circular thoughts, feelings, and actions. When the symptoms form a recognizable pattern, a doctor can diagnose and treat a person.
The emotions an individual feels on a daily basis dictate the type of person they feel they are. And yet it is a series of biological processes in the brain that generate every feeling a person has.
What is emotion?
Emotions impact hugely on people’s lives—they govern their behavior, give meaning to their existence, and are at the core of what it is to be considered human. Yet in reality emotions result from physiological responses in the brain triggered by different stimuli—the psychological significance read into emotions is an entirely human construct. Emotions evolved to promote human success and survival by initiating certain behaviors: for example, feelings of affection prompt the desire to find a mate, reproduce, and live in a group; fear generates a physiological response to avoid danger (fight-or-flight); reading emotions in others makes social bonding possible.
Processing emotion
The limbic system (p.26), located just under the cortex, generates all emotions. They are processed via two routes, conscious and unconscious (below). The primary receptor that “screens” the emotional content of all incoming stimuli is the amygdala, which signals to other areas of the brain to produce an appropriate emotional response. Connections between the limbic system and the cortex, in particular the frontal lobes, enable emotions to be processed consciously and experienced as valuable “feelings.” Each emotion is activated by a specific pattern of brain activity— hatred, for example, stimulates the amygdala (which is linked to all negative emotion) and areas of the brain associated with disgust, rejection, action, and calculation. Positive emotion works by reducing activity in the amygdala and those cortical regions linked to anxiety.
Conscious and unconscious emotive routes
Humans experience their emotional responses through an unconscious route, which is designed to prepare the body for rapid action (fight-or-flight), or via a conscious route, which enables a more considered response to a situation. The amygdala responds to threat and can detect stimuli before the person is even aware of it, provoking an automatic, unconscious reaction. A simultaneous, but slower, transmission of sensory information to the cortex creates a conscious secondary route for the same stimulus, and can modify this initial reaction.
Conscious
Thalamus All sensory information comes to the thalamus for distribution to the amygdala for quick assessment and action, and to the cerebral cortex for slower processing to conscious awareness.
Sensory cortex All sensory information comes to the sensory cortex for recognition. It extracts more information along this path, but the process takes longer than the unconscious route.
Hippocampus Consciously processed information is encoded in the hippocampus to form memories. The hippocampus also feeds back stored information, confirming or modifying the initial response.
CONSCIOUS FACIAL EXPRESSIONS
The motor cortex allows a person to control facial expression and so hide or express genuine emotion.
unconscious
Amygdala The amygdala instantly assesses incoming information for emotional content. It sends signals to other areas for immediate bodily action. It operates unconsciously and so is liable to make errors.
Hypothalamus Signals from the amygdala come to the hypothalamus, which triggers hormonal changes that make the body ready for “fight or flight” in response to emotional stimuli. The muscles contract and the heart rate increases.
REFLEX FACIAL EXPRESSIONS
The emotional reaction caused by the amygdala sparks spontaneous, uncontrolled facial expressions.
EMOTIVE BEHAVIORS AND RESPONSES
Typical behavioral patterns in response to emotion have evolved in order to neutralize any perceived threat, through either fight or appeasement. In contrast, moods last longer, are less intense, and involve conscious behaviors.
EVERY EMOTION sparks a slightly different pattern of activity in the brain.
“Human behavior flows from … desire, emotion, knowledge.”
Every experience generates a memory—whether it lasts depends on how often it is revisited. Intricate neural connections allow memories to form, and these can strengthen, aiding recall, or fade away.
What is memory?
A memory is formed when a group of neurons fire in a specific pattern in response to a new experience— these neural connections can then refire in order to reconstruct that experience as a memory. Memories are categorized into five types (right). They are briefly stored in the short-term (working) memory but can fade unless the experience is of emotional value or importance,in which case it is encoded (below) in the long-term memory. In recalling a memory, the nerve cells that first encoded it are reactivated. This strengthens their connections and, if done repeatedly, solidifies the memory. A memory’s component parts, such as related sounds or smells, reside in different areas of the brain, and in order to retrieve the memory all of these brain parts must be activated. During recall a memory can merge accidentally with new information, which fuses irrevocably with the original (known as confabulation). Endel Tulving explained memory as two distinct processes: storing information in long-term memory, and retrieving it. The link between the two means that being reminded of the circumstances in which a memory was stored can act as a trigger to recall the memory itself.
TYPES OF MEMORY
❯ Episodic memory Recalling past events or experiences, usually closely linked with sensory and emotional information.
❯ Semantic memory Retaining factual information, such as the name of a capital city.
❯ Working memory Storing information temporarily; capable of holding between five and seven items at any one time; also known as short-term memory.
❯ Procedural (body) memory Using learned actions that require no conscious recall, such as riding a bicycle.
❯ Implicit memory Bringing back an unconscious memory that influences behavior, such as recoiling from a stranger reminiscent of someone unpleasant.
CASE STUDY: BADDELEY’S DIVERS
Studies by psychologists indicate that in retrieving memories humans are aided by memory cues. British psychologist Alan Baddeley conducted an experiment in which a group of divers were asked to learn a list of words—they learned some words on dry land and some underwater. When they were later asked to recall the words, most divers found recall easier in the physical environment in which they had first memorized them, so it was easier to remember the words learned underwater when they went underwater. Baddeley’s experiment suggested that context itself could provide a memory cue. Similarly, when a person goes to collect an object from another room but on arriving cannot recall what they were looking for, often returning to the original room triggers that memory cue.
How memories form
The process of laying down (encoding) a memory depends on many factors. Even once encoded a memory can take two years to be firmly established.
1. Attention Focusing attention on an event helps to solidify the memory: the thalamus activates neurons more intensely, while the frontal lobe inhibits distractions.
2a. Emotion High emotion increases attention, making an event more likely to be encoded into a memory. Emotional responses to stimuli are processed in the amygdala.
2b. Sensation Sensory stimuli are part of most experiences, and if of high intensity they increase the chances of recollection. Sensory cortices transfer signals to the hippocampus.
3. Working memory Short-term memory stores information until needed—it is kept active by two neural circuits that incorporate the sensory cortices and the frontal lobes
4. Hippocampal processing Important information transfers to the hippocampus, where it is encoded. It can then loop back to the brain area that first registered it, to be recalled as a memory.
5. Consolidation The neural firing patterns that encode an experience carry on looping from the hippocampus to the cortex—this firmly fixes (consolidates) it as a memory.
“Memory is the treasury and guardian of all things.”
Studies of the brain have given valuable insight into the vital correlation between brain activity and human behavior, as well as revealing the complex process by which the brain itself is brought to life.
Connecting brain and behavior
Understanding the biology of the brain and how it works became vital with the rise of neuroscience in the 20th century. Studies in this field confirmed that the brain itself is fundamentally intertwined with human behavior, and prompted the emergence of specialist fields, such as neuropsychology. This relatively new branch of science combines cognitive psychology (the study of behavior and mental processes) with brain physiology, and examines how specific psychological processes relate to the brain’s physical structure. Investigating the brain in this light raises the age-old question of whether mind and body can be separated. The relationship between brain and mind has been debated since the time of ancient Greece and Aristotle, when prevailing philosophical thought labeled the two entities as distinct. This theory, which René Descartes reiterated in the 17th century with his concept of dualism (right), permeated studies of the brain until well into the 20th century. Modern neurological research and advances in technology have enabled scientists to trace certain behaviors to specific areas of the brain, and to study connections between the different regions. This has radically advanced knowledge of the brain and its effect on behavior, mental function, and disease.
Mind controlling brain
Dualism argues that the nonphysical mind and the physical brain exist as separate entities, but are able to interact. It considers that the mind controls the physical brain, but allows that the brain can at times influence the normally rational mind, for example, in a moment of rashness or passion.
Brain controlling mind
Monoism recognizes every living thing as material, and that the “mind” is therefore purely a function of the physical brain. All mental processes, even thoughts and emotions, correlate to precise physical processes in the brain. Cases of brain damage reinforce this: minds alter when the physical brain is altered.
“I think, therefore I am.”
René Descartes, French philosopher
Mind-body dualism
Humans are innately reluctant to reduce consciousness to pure biology. But the scientific evidence shows that the physical firing of neurons generates our thoughts. Two schools of thought, monoism and dualism, dominate the question of whether the mind is part of the body, or the body part of the mind.
SPECIALIZATION OF THE CEREBRAL HEMISPHERES
CEREBRAL CORTEX
Nerve fibers cross over at the base of the brain, so each hemisphere controls the opposite side of the body.
Left hemisphere
❯ This controls and coordinates the right side of the body.
❯ It is the analytical side of the brain.
❯ It is responsible for tasks relating to logic, reasoning, decision-making, and speech and language.
Right hemisphere
❯ This controls muscles on the left side of the body.
❯ It is the creative side of the brain.
❯ It deals with sensory inputs, such as visual and auditory awareness, creative and artistic abilities, and spatial perception.
Mapping the brain
One of the most complex systems in nature, the human brain controls and regulates all our mental processes and behaviors, both conscious and unconscious. It can be mapped according to its different neurological functions, each of which takes place in a specific area. The hierarchy of mental processing is loosely reflected in the brain’s physical structure: high-level cognitive processes take place in the upper areas, while more basic functions occur lower down. The largest and uppermost region (the cerebral cortex) is responsible for the highest-level cognitive function, including abstract thought and reasoning. It is the capacity of their cerebral cortex that separates humans from other mammals. The central limbic areas (below) control instinctive and emotional behavior, while structures lower in the brain stem maintain vital bodily functions, such as breathing.
Functional divisions
The cerebral cortex (also called the cerebrum) divides into two separate but connected hemispheres, left and right. Each one controls a different aspect of cognition . Further divisions include four paired lobes (one pair on either hemisphere), each of which is associated with a specific type of brain function.The frontal lobe is the seat of high-level cognitive processing and motor performance; the temporal lobe is involved in short- and long-term memories; the occipital lobe is associated with visual processes; and the parietal lobe deals with sensory skills. Brain-imaging techniques, such as fMRI (functional magnetic resonance imaging), measure activity in the different brain areas, yet their value to psychologists can be limited. Those studying fMRI results need to be aware, for example, of the issue of “reverse inference”: just because a particular part of the brain is shown to be active during one cognitive process does not mean it is active because of that process. The active area might simply be monitoring a different area, which is in fact in control of the process.
The limbic system
This complex set of structures is involved in processing emotional responses and the formation of memories.
Hypothalamus Involved in regulating body temperature and water levels and key behavioral responses.
Olfactory bulb Relays messages about smell to the central limbic areas for processing.
Amygdala Processes emotions; affects learning and memory.
Hippocampus Converts short-term memories into long-term ones.
Thalamus Processes and sends data to higher brain areas.
Locating brain function
Psychologists and neurologists can map neurological function when small areas of the brain are stimulated. Using brainscanning techniques, such as fMRI or CT, they study and record the sensation and movements this stimulation produces.
Broca’s area
Dorsolateral prefrontal cortex This area is linked to various high-level mental processes, including “executive functions”— the processes involved in self-regulation or mental control.
OFC (orbital frontal cortex) Part of the prefrontal cortex, the OFC connects with the sensory and limbic areas; it plays a role in the emotional and reward aspect of decision-making.
FRONTAL LOBE
Supplementary motor cortex One of the secondary motor cortices, this area is involved in planning and coordinating any complex movements. It sends information to the primary motor cortex.
Wernicke’s area
Plays a key role in the comprehension of spoken language.
Tempo-parietal junction Located between the temporal and parietal lobes, this area processes signals from limbic and sensory areas, and has been linked with the comprehension of “self.”
Cerebellum
Brain stem Main control center for key bodily functions, such as swallowing or breathing.
OCCIPITAL LOBE
Primary visual cortex Visual stimuli are initially processed in this cortex, enabling recognition of color, movement, and shape. It sends signals on to other visual cortices to be processed further.
PARIETAL LOBE
Motor cortex This is the primary area of the cerebral cortex involved in motor function. It controls voluntary muscle movements, including planning and execution.
Sensory cortex Information gathered by all five senses is processed and interpreted here. Sensory receptors from around the body send neural signals to this cortex.
Lighting up the brain
The human brain contains around 86 billion specialized nerve cells (neurons) that “fire” chemical and electrical impulses to allow communication between them and the rest of the body. Neurons are the core building blocks of the brain, and connect to form complex pathways through the brain and central nervous system. Neurons separate at a narrow junction called a synapse. In order to pass a signal on, the neuron must first release biochemical substances, known as neurotransmitters, which fill the synapse and activate the neighboring cell. The impulse can then flow across the synapse in a process known as synaptic transmission. In this way the brain sends messages to the body to activate the muscles, and the sensory organs are able to send messages to the brain.
Forming pathways
transmission indicate that pathways within this vast network link to specific mental functions. Every new thought or action creates a new brain connection, which strengthens if it is used repeatedly, and it is then more likely that the cells will communicate along that pathway in the future. The brain has “learned” the neural connections associated with that particular activity or mental function.
86 billion neurons exist in the brain
Acetylcholine The effects of this neurotransmitter are mostly excitatory, and activate the skeletal muscles; it is also linked to memory, learning, and sleep.
Glutamate The most common neurotransmitter, glutamate has an excitatory effect and links to memory and learning.
GABA The brain’s main inhibitory neurotransmitter, GABA slows the firing of neurons and is calming.
Adrenaline Released in stress situations, adrenaline creates an energy surge that increases heart rate, blood pressure, and blood flow to the larger muscles.
Endorphins Released by the pituitary gland, endorphins have an inhibitory effect on the transmission of pain signals; they are associated with pain relief and feelings of pleasure.
Serotonin With an inhibitory effect, serotonin is linked to mood enhancement and calmness. It regulates appetite, temperature, and muscle movement.
Norepinephrine Similar to adrenaline, this excitatory neurotransmitter is mainly associated with the fight-or-flight mechanism; it is also linked to stress resilience.
Dopamine With either an inhibitory or an excitatory effect, dopamine plays a key role in rewardmotivated behavior and links to mood.
Neurotransmitters
Many different types of neurotransmitters are released at a synapse, and may have either an “excitatory” or an “inhibitory” effect on a target cell. Each type is linked with a specific brain function, such as regulating mood or appetite. Hormones have a similar effect but are transmitted by blood, whereas neurotransmitters are transmitted across the synaptic cleft.
CHEMICAL EFFECTS AND OVERLAPS
These three neurotransmitters have distinct yet interrelated roles.
❯ All affect mood.
❯ Norepinephrine and dopamine are both released in stressful situations.
❯ Serotonin moderates a neuron’s response to the excitatory effects of dopamine and norepinephrine.
Based on the premise that physical factors, such as genes, determine behavior, this approach can explain how twins brought up separately exhibit parallel behavior.
What is it?
Biological psychology assumes that people’s thoughts, feelings, and behavior all derive from their biology, which includes genetics as well as the chemical and electrical impulses that wire the brain to the nervous system. This assumption implies that the blueprint laid down in the womb—people’s physiological structure and DNA—dictates their personality and behavior as they go through life. Some of these ideas are based on the results of twin studies, which have shown that twins separated at birth and brought up in different households display remarkably similar behavior in adult life. Biopsychologists argue that this phenomenon can be explained only if the twins’ genetics influence them so strongly that not even the role of their parents, friends, life experiences, or environment have much impact. An example of biological psychology in action is the research into how teenagers behave. Scans of teenage brains using imaging technology have revealed that adolescent brains process information in a different way than adult brains. These differences help to offer a biological explanation for why teenagers can be impulsive, sometimes lack good judgment, and can become overly anxious in social situations.
Evaluation
Many of the ideas in biological psychology emphasize nature over nurture. As a result, critics consider the approach to be oversimplistic, giving undue weight to the influence of biology and built-in physical attributes. Little credit is given to the influence of events or people on an individual as they grow up. On the other hand, few argue with the rigorous scientific backbone of the approach, which places importance on the systematic testing and validation of ideas. And biopsychologists have enabled important medical advances—using research from neurosurgery and brain imaging scans, they have made positive contributions to treatment for patients with both physical and mental problems, including Parkinson’s disease, schizophrenia, depression, and drug abuse.
EVOLUTIONARY PSYCHOLOGY
Psychologists in this field explore why people’s behavior and personality develop differently. They investigate how individuals adapt their language, memory, consciousness, and other complex biological systems to best cope with the environment they find themselves in. Key ideas include:
❯ Natural selection This has its origins in Charles Darwin’s hypothesis that species adapt over time or evolve mechanisms that facilitate survival.
❯ Psychological adaptations This looks at mechanisms people use for language acquisition, for differentiating kin from non-kin, for detecting cheats, and for choosing a mate based on certain sexual or intelligence criteria.
❯ Individual differences This seeks to explain the differences between people—for example, why some people are more materially successful than others.
❯ Information processing This evolutionary view suggests that brain function and behavior have been molded by information taken in from the external environment, and so are the product of repeatedly occurring pressures or situations.
Different approaches
Physiological This approach is based on the assumption that biology shapes behavior. It seeks to discover where certain types of behavior originate in the brain, how hormones and the nervous system operate, and why changes in these systems can alter behavior.
Medical This branch explains and treats mental disorders in terms of physical illness. Disorders are considered to have a biological basis, such as a chemical imbalance in the body or damage to the brain, rather than causes linked to environmental factors.
Genetics This field attempts to explain behavior in terms of patterns that are laid down in each person’s DNA. Studies of twins (especially twins separated at birth and raised in different homes) have been used to show that traits such as IQ are inherited.
“In the last analysis the entire field of psychology may reduce to biological electrochemistry.”
A branch of psychology that considers the mind to be like a complex computer, the cognitive approach analyzes the way people process information and how that dictates their behavior and emotions.
What is it?
When the computer arrived in offices in the late 1950s, it sparked comparisons between artificial information processing and the operation of the human mind. Psychologists reasoned that in the same way that a computer accepts data, codes it for storage, and retrieves it, the human mind takes in information, changes it to make sense of it, stores it, and recalls it when needed. This computer analogy came to be the foundation for cognitive psychology. The theories behind cognitive psychology can apply to virtually every aspect of daily life. Examples include the brain receiving and processing sensory information to make a judgment (such as recognizing that a carton of milk has soured from its bad smell); reasoning with logic to reach a decision (such as whether to buy an expensive shirt that may last longer than a cheap one); or learning how to play a musical instrument, which requires the brain to make new connections and store new memories.
Evaluation
Although cognitive psychology emphasizes internal processes, it aims to be strictly scientific, relying on laboratory experiments to back up any theory. What happens in controlled experiments, however, can be difficult to apply to real-life scenarios. Similarly, the assumption that the human mind functions like a computer does not take into account realities such as people getting tired and emotional, and critics claim it treats humans as machines, reducing all behavior to a cognitive process such as committing things to memory. Critics have also pointed out that this approach ignores the roles of biology and genetics. However, cognitive psychology has proved useful for treating memory loss and selective attention disorders. It is also valuable in understanding child development, allowing educators to plan appropriate content for each age group, and to decide the best tools for delivering it. In the legal system, cognitive psychologists are regularly called on to assess eyewitness reports in order to determine whether a witness has accurately recalled a crime.
Information processing
Using evidence from controlled experiments, psychologists have built theoretical models of how the mind deals with information. According to these models, the human brain handles information in the same sequence a computer uses to handle data—from input, through transformation of the data, to retrieval.
INPUT (from environment)
A person’s sense organs detect stimuli from the external world and send messages to the brain as electrical impulses containing information. For example, if a person’s car breaks down, their brain focuses on warning signs, such as unexpected sounds from the engine, visual cues like smoke, or the smell of burning rubber.
PROCESSING (mediational mental event)
After receiving information via the senses, the brain must sort through it to analyze it and decide what to do with it. Cognitive psychologists call this process mediational because it happens between (“mediates”) the environmental stimulus and the brain’s eventual response to that stimulus. In the case of a car breakdown, the brain might analyze the smell of burning rubber, and connect it with an earlier memory of a similar smell.
OUTPUT (behavior and emotion)
When the brain has retrieved enough information, it can make a decision about what response to make, in the form of either a behavioral or an emotional reaction. In the example of the car, the brain recalls memories of previous breakdowns, together with any relevant mechanical information stored, and then runs through a mental checklist of possible causes and solutions. It remembers that the smell of burning rubber previously indicated a broken fan belt. The person pulls over, turns off the ignition, and opens the hood to check.
“Disconnected facts in the mind are like unlinked pages on the Web: they might as well not exist.”
Steven Pinker, Canadian cognitive psychologist
COGNITIVE BIAS
When the mind makes an error in the course of thought processing, it results in a skewed judgment or reaction, known as a cognitive bias. This may be related to memory (poor recall, for example) or lack of attention, usually because the brain is making a mental shortcut under pressure. Biases are not always bad—some are the natural outcome of having to make a quick decision for survival purposes.
Examples of bias
❯ Anchoring Placing too much importance on the first piece of information heard.
❯ Base-rate fallacy Abandoning original assumptions in favor of a new piece of information.
❯ Bandwagon effect Overriding own beliefs in order to go along with what other people are thinking or doing.
❯ Gamblers’ fallacy Mistakenly believing that if something is happening more often now, it will happen less often in the future— for example, if the roulette wheel consistently falls on black, thinking it is bound to fall on red before long.
❯ Hyperbolic discounting Choosing a smaller reward now, rather than patiently waiting for a larger reward.
❯ Neglect of probability Disregarding true probability, for example, avoiding air travel for fear of a plane crash, but fearlessly driving a car even though it is statistically far more dangerous.
❯ Status quo bias Making choices to keep a situation the same or alter it as little as possible, rather than risking change.
Unlike other psychological approaches, humanism places central importance on the individual’s viewpoint, encouraging the question “How do I see myself?” rather than “How do others see me?”
What is it?
Whereas behavioral psychology is concerned with observing external actions and psychoanalysis delves into the subconscious, humanism is holistic, focusing on how a person perceives their own behavior and interprets events. It centers on a person’s subjective view of themselves and who they would like to be, rather than the objective view of an observer. Pioneered by Carl Rogers and Abraham Maslow in the 1950s, humanism offers an alternative way of trying to fathom human nature. It assumes that personal growth and fulfillment are primary goals in life, and that emotional and mental well-being comes from achieving this. The principle of free will, exercised in the choices a person makes, is also key.
“The good life is a process, not a state of being.”
Carl Rogers, American humanist psychologist
Evaluation
Rogers and other humanist psychologists suggested a number of new methods of investigation, such as open-ended questionnaires in which there were no “right” answers, casual interviews, and the use of diaries to record feelings and thoughts. They reasoned that the only way to really get to know someone was to talk to them. Humanism is the theory that underpins person-centered therapy (p.132)—one of the most common therapies for depression. The humanistic approach is also used in education to encourage children to exercise free will and make choices for themselves, and in researching and understanding motivation. However, humanism ignores other aspects of the individual such as their biology, the subconscious mind, and the powerful influence of hormones. Critics also say that the approach is unscientific, because its goal of self-realization cannot be accurately measured.
Road to fulfillment
INCONGRUENT
INCREASINGLY CONGRUENT
SELF-ACTUALIZATION
GESTALT PSYCHOLOGY
Influenced by humanism, gestalt psychology examines in detail how the mind takes small pieces of information and builds them into a meaningful whole. It emphasizes the importance of perception—the laws that govern how each person perceives the world. Part of gestalt assessment involves showing clients a series of images to discover how their eye perceives each one. The Rubin Vase illusion is the best known of these, and illustrates the law of “figure” and “ground”: a person’s mind always works to distinguish a figure (words, for example) from its background (a white page), and in doing so, makes a decision about priority and what to focus on.
THE RUBIN VASE ILLUSION offers the viewer a perceptual choice between seeing two faces in profile and seeing a white vase.
INDIVIDUAL OR GROUP?
Humanism is rooted in Western ideas of personal identity and achievement, sometimes called individualism. In contrast, collectivism subordinates the person to the group.
Individualism
❯ Identity defined in terms of personal attributes— such as outgoing, kind, or generous
❯ Own goals take priority over those of the group
Collectivism
❯ Identity defined by which group someone belongs to❯ Family, then workplace, are most important groups
Behavioral psychology analyzes and treats people on the basis that their behavior is learned by interacting with the world and that the influence of the subconscious is irrelevant.
What is it?
The starting point for behavioral psychology is a focus on only observable human behavior, leaving out thought and emotion. This approach rests on three main assumptions. First, people learn their behavior from the world around them, and not from innate or inherited factors. Second, because psychology is a science, measurable data from controlled experiments and observation should support its theories. Third, all behavior is the result of a stimulus that triggers a particular response. Once the behavioral psychologist has identified a person’s stimulus-response association, they can predict it, a method known as classical conditioning (below). In therapy , the therapist uses this prediction to help the client change their behavior.
Evaluation
The strength of the behaviorist approach—that it can be scientifically proven, unlike Freud’s psychoanalytic approach , for example—has also been seen as its weakness. Many of the behavioral experiments were carried out on rats and dogs, and humanists (min particular rejected the assumption that people in the world acted in the same way as animals in laboratory conditions. Behavioral psychology also takes little account of free will or biological factors such as testosterone and other hormones, reducing human experience to a set of conditioned behaviors.
OPERANT CONDITIONING
This method for inducing behavior change, in this case training a dog, involves positive or negative actions on the part of the owner to reinforce or punish the dog’s behavior.
❯ Positive reinforcement Giving a reward encourages good behavior. For example, the dog receives a treat for sitting on command. It quickly learns that repeating that behavior will earn it another treat.
❯ Negative reinforcement The owner removes something bad to encourage good behavior. The lead goes slack when the dog walks close to its owner. The dog learns to walk to heel without pulling and so avoid the choking sensation.
❯ Positive punishment The owner does something unpleasant to discourage bad behavior. When the dog pulls ahead on the lead, its collar feels uncomfortably tight around its throat.
❯ Negative punishment Taking away something that the dog enjoys is used to discourage undesired behaviors. For example, the owner turns their back on the dog to deprive it of attention if it jumps up. The dog learns not to jump up.
Themes of behaviorism
John Watson developed behavioral psychology in 1913. His theory agreed with the early 20th-century trend toward data-backed science rather than concentrating on the subjective workings of the mind, and the behaviorist approach was influential for decades. Later psychologists interpreted behavioral theory along more flexible lines, but objective evidence remains a cornerstone of research.
METHODOLOGICAL BEHAVIORISM
Watson’s theory became known as methodological behaviorism because of its focus on scientific methods:
❯ He viewed psychology as a science, its goals being the prediction and control of behavior.
❯ It is the most extreme theory of behaviorism because it rules out any influence from a person’s DNA or internal mental state. Neutral stimulus Unconditioned response Unconditioned stimulus Conditioned stimulus Conditioned response EXTERNAL
❯ It assumes that when people are born their minds are a blank slate and they learn all their behavior from the people and things around them (classical conditioning, left). For example, a baby smiles back when their mother smiles, or cries if their mother raises her voice.
RADICAL BEHAVIORISM
In the 1930s B. F. Skinner developed radical behaviorism, which allowed for the influence of biology on behavior:
❯ Like Watson, Skinner believed that the most valid approach to psychology was one based on scientifically observing human behavior and its triggers.
❯ Skinner took classical conditioning a step forward with the idea of reinforcement— behavior that is reinforced by a reward is more likely to be repeated (operant conditioning, above).
PSYCHOLOGICAL BEHAVIORISM
Conceived by Arthur W. Staats, psychological behaviorism gained dominance over four decades. It informs current practice in psychology, especially in education:
❯ A person’s personality is shaped by learned behaviors, genetics, their emotional state, how their brain processes information, and the world around them.
❯ Staats researched the importance of parenting in child development
❯ He showed that early linguistic and cognitive training resulted in advanced language development and higher performance in intelligence tests when children were older.
This psychological theory proposes that the unconscious struggles of the mind determine how personality develops and dictates behavior.
What is it?
What is it? Founded by Austrian neurologist Sigmund Freud in the early 20th century, psychoanalytical theory proposed that personality and behavior are the outcome of continual conflicts in the mind. The individual is not usually aware of the discord because it takes place at a subconscious level. Freud suggested conflict occurs between three parts of the mind: the id, superego, and ego (below, right). Freud believed that personality develops from birth in five stages, which he called psychosexual because they involve both sexuality and mental processes. At each stage a person’s mind focuses on a different aspect of sexuality, such as oral pleasure when they suck their thumb as a baby. Freud believed that the psychosexual stages trigger a battle between biology and social expectations, and the mind must resolve this conflict before a person can move on to healthy mental development.
Evaluation
Although Freud’s model has been hugely influential in highlighting the role of the subconscious , it has proved controversial because it focuses on sexuality as the driver of personality. Many critics view his model as too subjective and too simplistic to explain the complex nature of the mind and behavior.
Topographical model
Freud divided the mind into three levels of consciousness. The conscious mind forms only a small part of the whole. Although it is completely unaware of the thoughts in the unconscious mind, the latter still affect behavior.
Psychoanalysis In this therapy , the client tells the analyst about their childhood memories and dreams in order to unlock the unconscious mind and reveal how it is controlling or triggering undesirable behavior.
Conscious mind This contains the ideas and emotions that people are aware of.
Preconscious mind This stores information such as childhood memories, which can be accessed through psychoanalysis.
Unconscious mind This hides most of a person’s impulses, desires, and thoughts.
Dreams Dreams are seen as a channel for unconscious thoughts that people cannot usually access because many of them are too disturbing for the conscious mind to cope with.
Structural model
The conscious mind is just the tip of the iceberg, a small part of a hidden whole. Psychoanalytical theory is based on the concept that the unconscious mind is structured in three parts—the id, ego, and superego—which “talk” to one another to try to resolve conflicting emotions and impulses.
NEED TO KNOW
❯ Inferiority complex When self-esteem is so low that a person cannot function normally. The idea was developed by neo-Freudian Alfred Adler.
❯ Pleasure principle What drives the id—the desire to obtain pleasure and avoid pain.
❯ Neo-Freudians Theorists who built on Freud’s psychoanalytic theories, such as Carl Jung, Erik Erikson, and Alfred Adler.




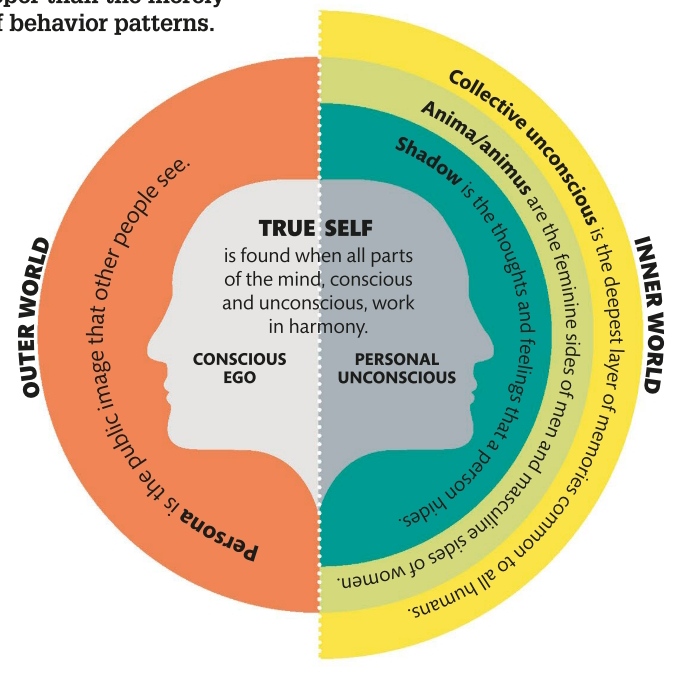

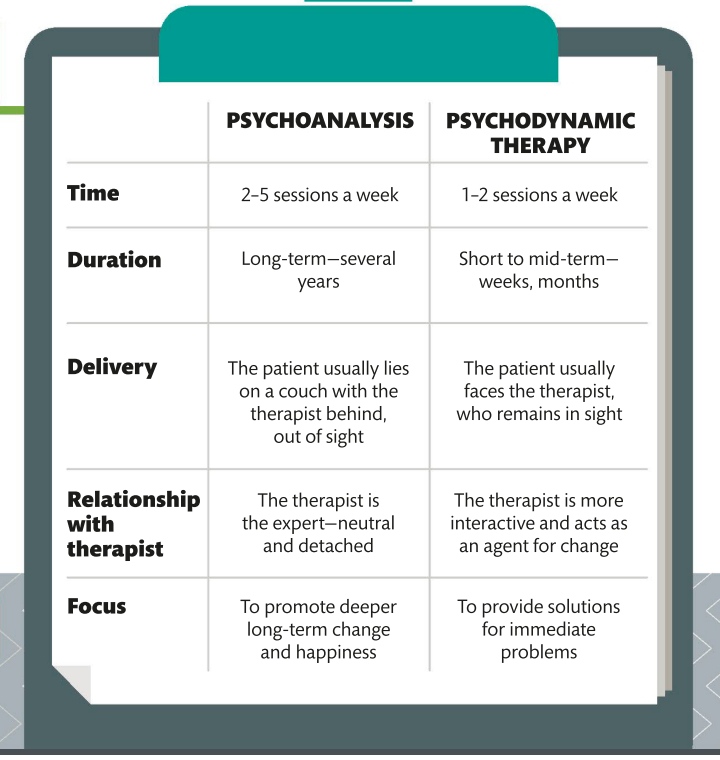


")


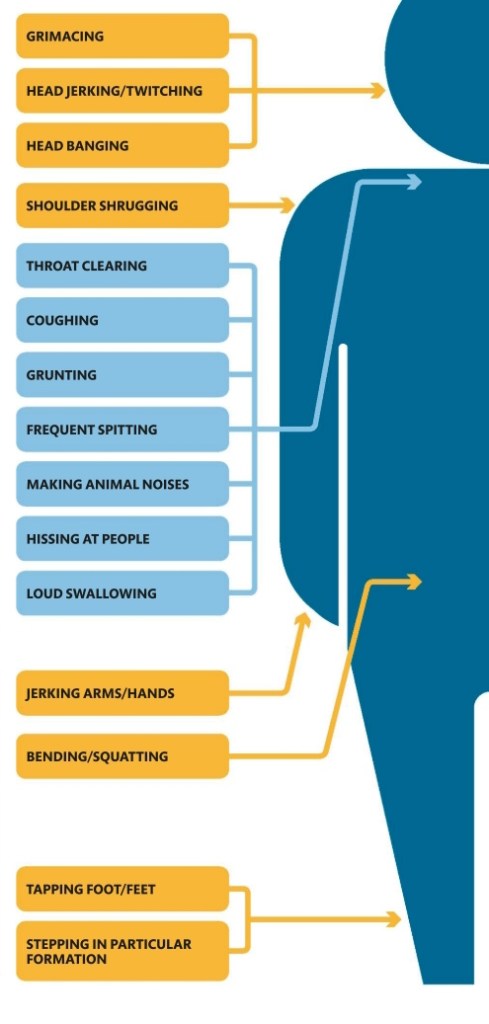
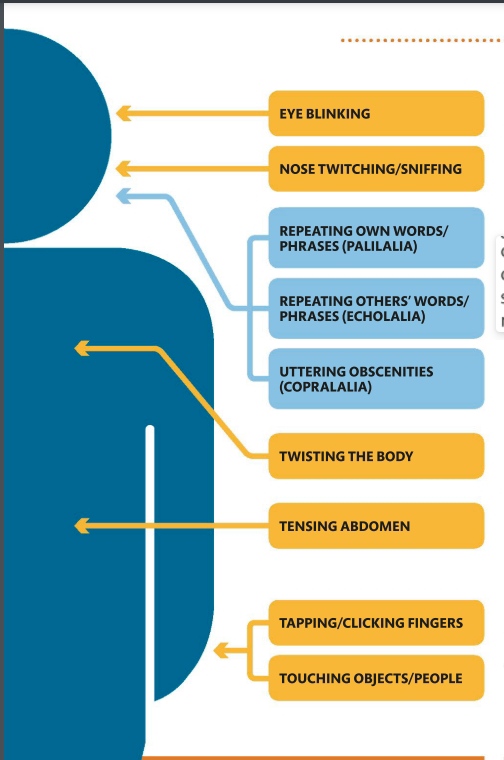

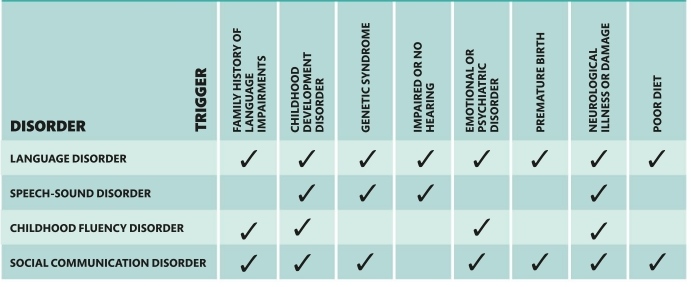

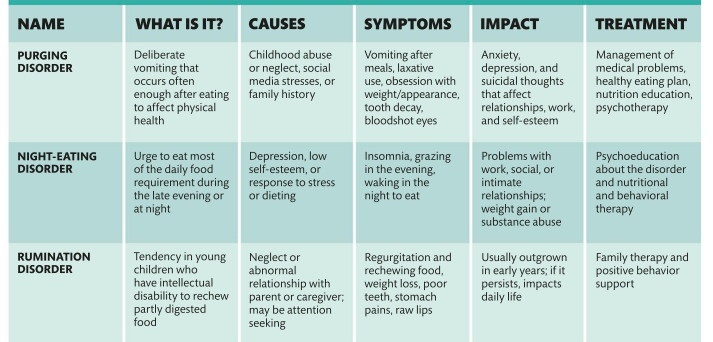

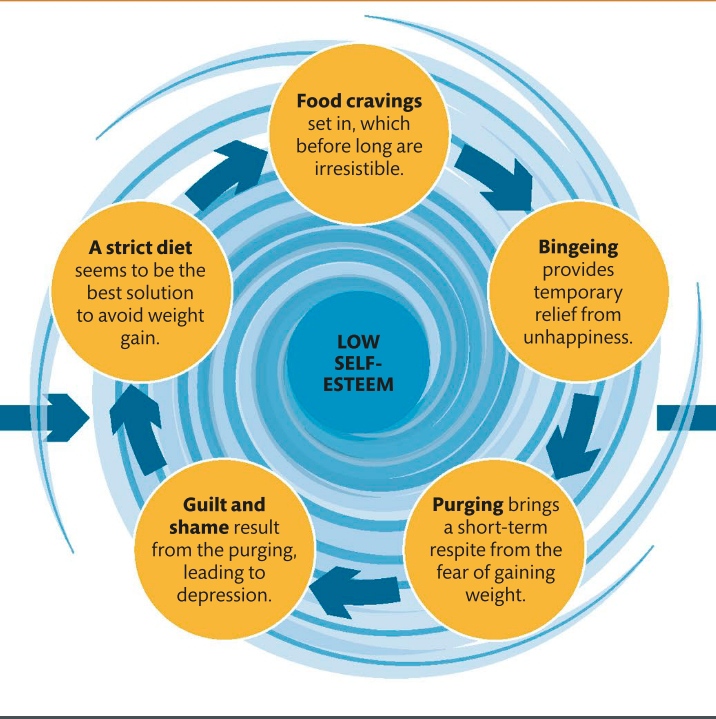


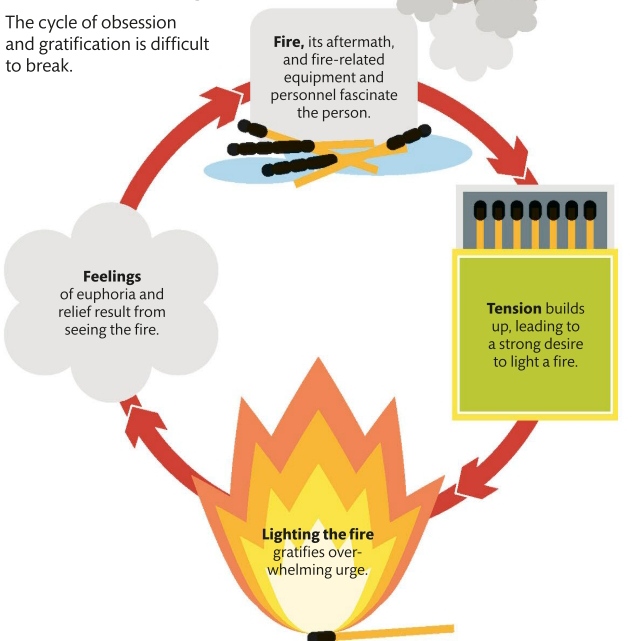

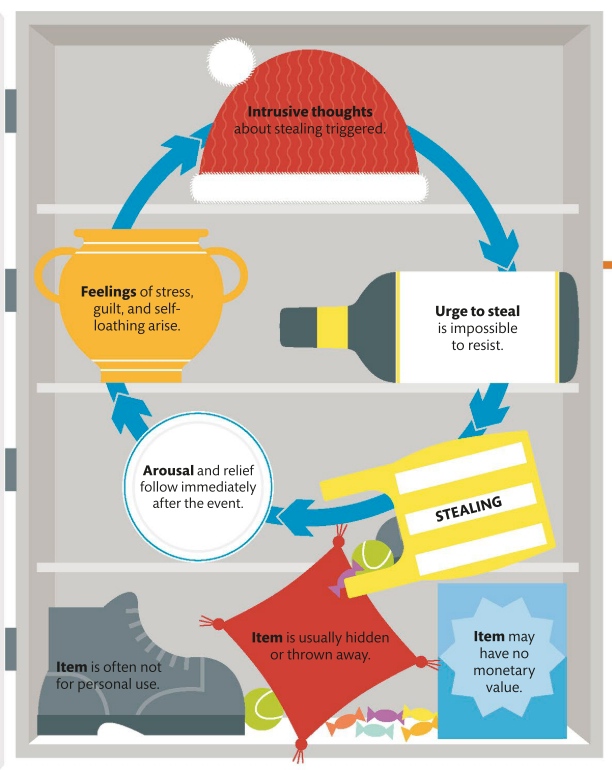




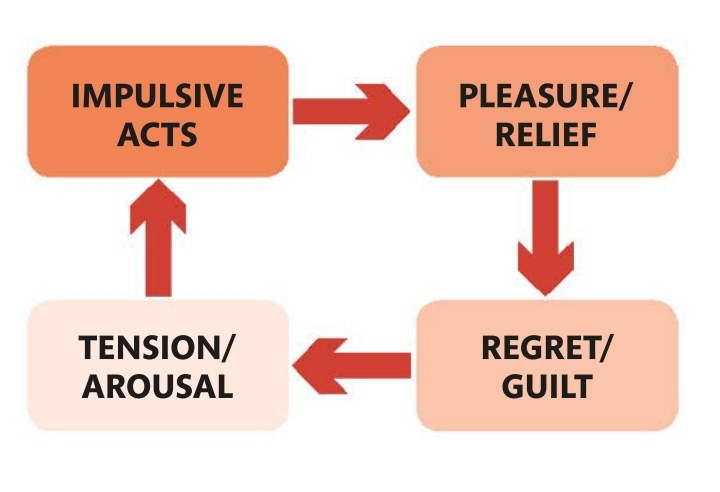
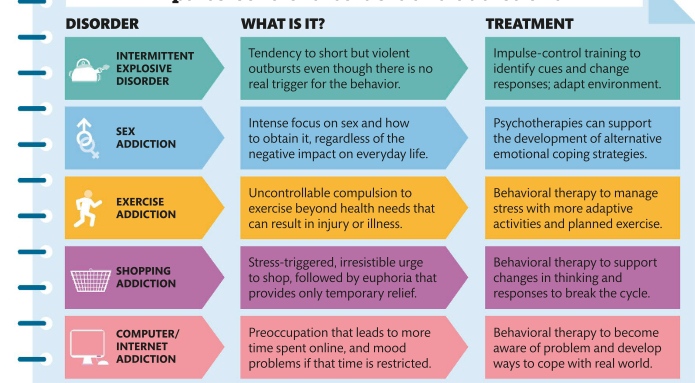
")
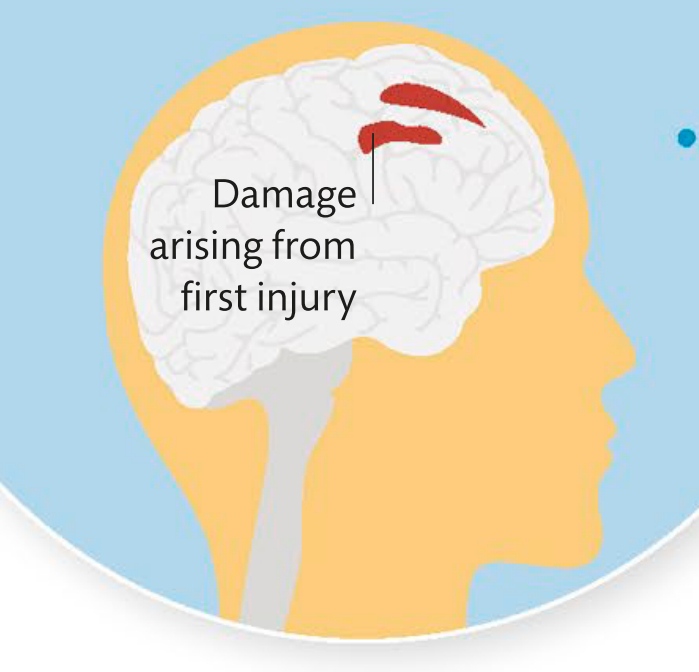





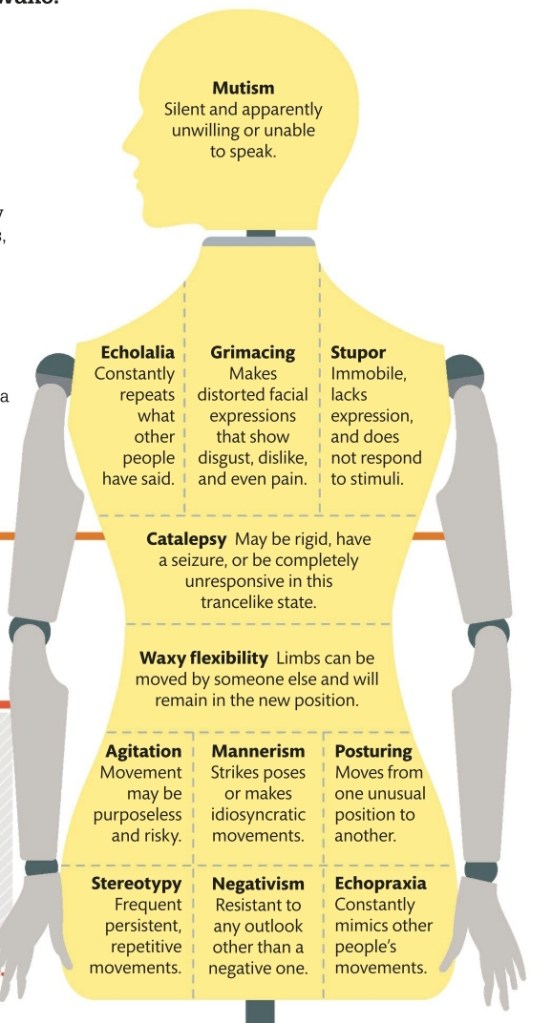

")
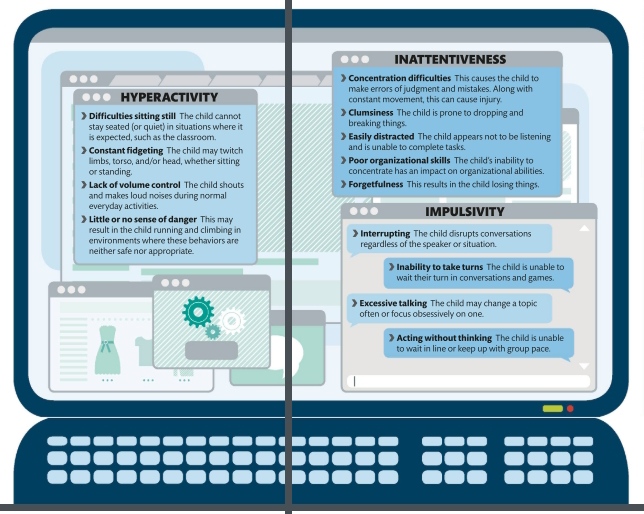

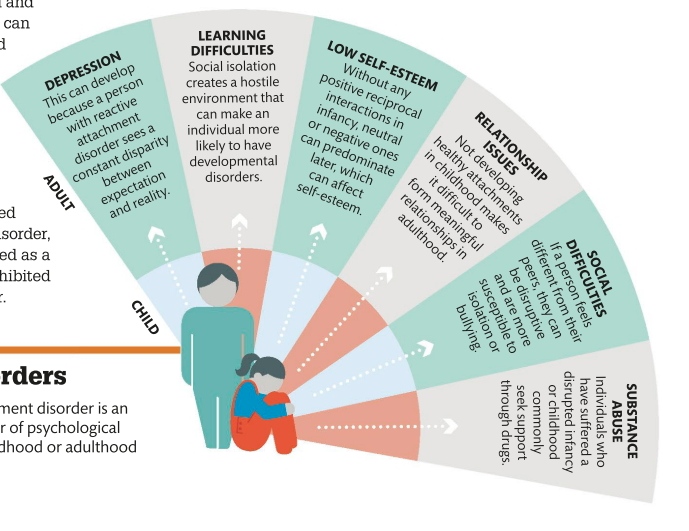

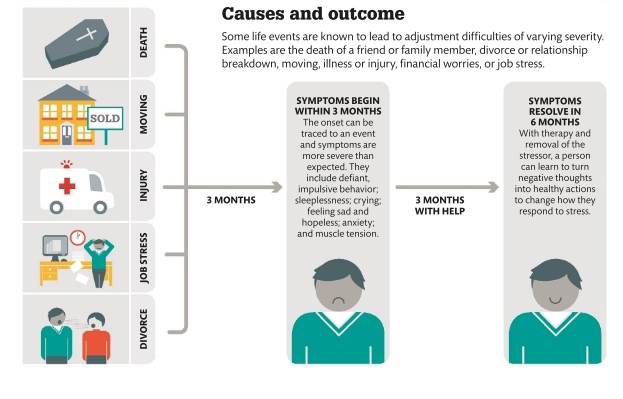
")
")


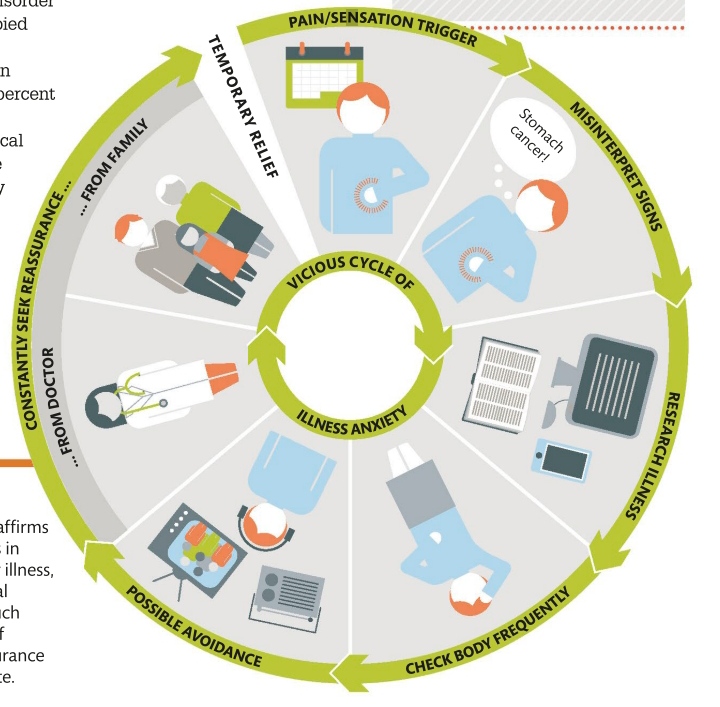

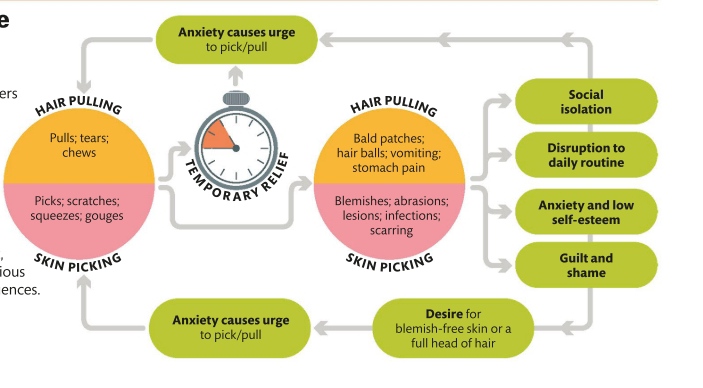


")
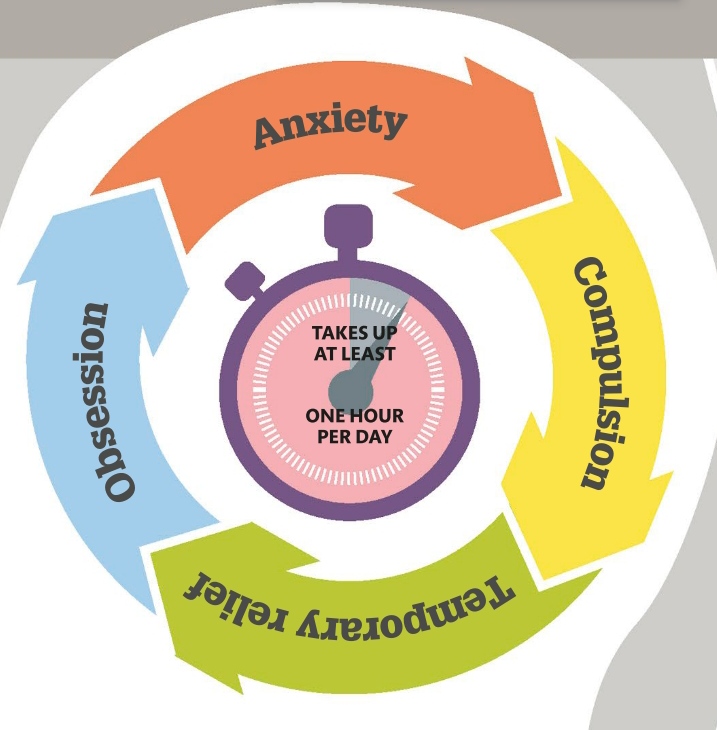











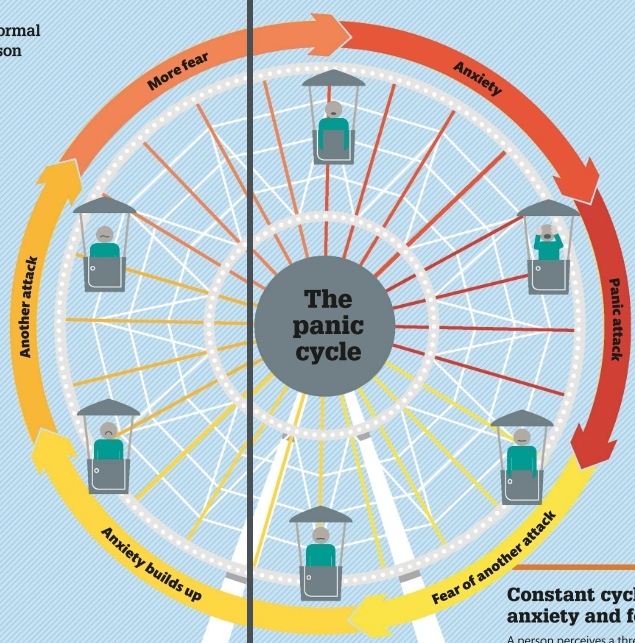
")
")