")
These are disorders in which individuals display persistent and consistent unhealthy patterns of thinking, behavior, and social functioning.
What are they?
Individuals with PD have difficulty not only understanding themselves, but also relating to other people. PD is different from other mental illnesses due to its enduring nature and the fact that it cannot be compared to a physical illness. The individual’s behavior varies noticeably from the norm in society, but they may manage their own life without medical help in a way that someone with an extreme condition such as schizophrenia cannot. PD often goes hand in hand with substance abuse , depression , and anxiety. The precise causes of personality
disorders are not known, but risk factors appear to include a family history of a personality or other mental disorder; an abusive, unstable, or chaotic early life; or a diagnosis of severe aggression and disobedience in childhood. Variations in brain chemistry and structure may also play a role. There are 10 defined PDs and
they are considered to fit into three clusters based on broad similarities within each group. A doctor does not usually attempt
a diagnosis of PD until early adulthood. For a diagnosis to be made, the symptoms must cause day-to-day problems with functioning and subjective distress, and the person must display some symptoms of at least one of the types.
Cluster A: odd/eccentric
A person with a Cluster A personality disorder shows patterns of behavior that most onlookers would regard as odd and eccentric, has difficulty relating to other people, and fears social situations. The individual may not believe that they have a problem. This group includes three personality disorders: paranoid, schizoid, and schizotypal.
Paranoid PD
- person is extremely distrustful and suspicious.
- ❯ They think other people are lying to them, trying to manipulate them, or passing on shared confidences.
- ❯ They find hidden meanings in innocent remarks.
- ❯ They have problems maintaining close relationships, often believing that a spouse or partner is unfaithful despite a lack of evidence, for instance.
- ❯ Their suspiciousness and hostility may be expressed in overt argumentativeness; recurrent complaining; or quiet, hostile aloofness.
- ❯ The person’s hypervigilance for potential threats makes them appear guarded, secretive, devious, and lacking in tender feelings.
Schizoid PD
- ❯ The person appears cold, detached, and indifferent to other people.
- ❯ They prefer to take part in activities alone.
- ❯ They have little desire to form close relationships of any kind, including sexual ones.
- ❯ They have a limited range of social expression.
- ❯ They cannot pick up social cues or respond to criticism or praise.
- ❯ They have limited ability to experience pleasure or joy.
- ❯ They are more likely to be male than female.
- ❯ They may have a relative with schizophrenia
Schizotypal PD
- ❯ The person becomes very anxious and introverted in social situations, even familiar ones.
- ❯ They make inappropriate responses to social cues.
- ❯ They have delusional thoughts, attaching undue and misguided significance to everyday events. For example, they may be convinced that a newspaper headline contains secret messages for them.
- ❯ They may believe in special powers such as telepathy or their own magical ability to influence another person’s emotions and actions.
- ❯ They may have unusual ways of speaking, such as making long, rambling, vague statements or changing the subject partway through.

PEOPLE WITH PD often do not see themselves as having a problem so seeking treatment is rare.
TREATMENT
❯ Paranoid PD Schema-focused cognitive therapy to enable links between problems, for example, emotions from childhood memories and current life patterns; also uses cognitive techniques to develop new appraisals. However, high dropout rates from treatment occur, even if sought, due to difficulty in building rapport and trust between therapist and patient.
❯ Schizoid PD Cognitive behavioral therapy or lifestyle support to reduce anxiety, depression, angry outbursts, and substance abuse; social skills training; medication prescribed for low mood or psychotic episodes. However, treatment is rarely sought.
❯ Schizotypal PD Long-term psychotherapy to build a trusting relationship and cognitive behavioral therapy to help with identification and reevaluation of irrational thoughts; medication prescribed for low mood or psychotic episodes.
Cluster B: dramatic/emotional/erratic
A person suffering from a Cluster B personality disorder struggles to regulate their feelings. They are usually overly emotional and unpredictable and display behavior patterns that others see as dramatic, erratic, threatening, and even disturbing. This creates a vicious cycle, as people are uncomfortable near them, so social and personal relationships are difficult to achieve and maintain, which in turn intensifies the initial symptoms.
PSYCHOPATHY
Sometimes considered a subset of antisocial personality disorder (below), psychopathy is one of the hardest disorders to diagnose and is largely resistant to treatment. Psychopathy presents as a specific set of personality traits and behaviors. Mental health professionals can use Robert Hare’s Psychopathy Checklist-Revised (PCL-R) to diagnose the disorder by scoring an individual on 20 listed traits with a value of 0, 1, or 2. A score of 30 and above in the US, or 25 and above in the UK, results in a diagnosis of psychopathy. Interpersonal traits include grandiosity, deceit, and arrogance; emotion-based traits, lack of guilt and empathy; and impulsive traits, sexual promiscuity as well as criminal behaviors such as stealing. Individuals lack inhibition and do not learn from experience. They can seem charming at first, but their inability to feel guilt, empathy, or love, along with the presence of casual, reckless attachments and behavior, quickly becomes evident. Many traits—especially the ability to make clear, emotion-free decisions—can be found in successful individuals, particularly in business and sports. Most psychopaths are men, and the disorder is unrelated to the society or culture they come from.
- Antisocial PD
- ❯ The person manipulates, exploits, or violates the rights of others.
- ❯ They see other people as vulnerable and may intimidate or bully them without remorse. They can be aggressive, even violent.
- ❯ Their behavior is often criminal; they lie and steal, and use aliases to deceive people.
- ❯ They disregard their own and others’ safety.
- ❯ They are consistently irresponsible and impulsive and have no concern for the consequences of their actions.
- ❯ They blame other people for problems they encounter.
- ❯ The disorder becomes evident in late teens and often dissipate by middle age.
Borderline pd
- ❯ The person has a fragile self-image.
- ❯ They are emotionally unstable (also called affect dysregulation), with severe mood swings and frequent, intense displays of anger.
- ❯ They have intense but unstable relationships with other people.
❯ They fear being alone or abandoned and have long-term feelings of emptiness and loneliness, leading to irritability, anxiety, and depression.
❯ They have disturbed patterns of thinking or perception (called cognitive or perceptual distortions). - ❯ They act impulsively, with a tendency to self-harm and suicidal thoughts
Histrionic PD
- ❯ The person is self-centered and regularly seeks attention.
- ❯ They dress or behave inappropriately, and draw attention to themselves through physical appearance.
- ❯ Their emotional states rapidly shift, which makes them appear shallow.
❯ They are excessively dramatic, with exaggerated displays of emotion.
❯ They constantly seek reassurance or approval. - ❯ They are suggestible (easily influenced).
- ❯ They believe that their relationships are more intimate than they are.
- ❯ They may function at a high level in social and work environments.
Narcissistic PD
- ❯ The person has an exaggerated sense of selfimportance, expects to be recognized as superior, and exaggerates their talents.❯ They are preoccupied with fantasies about success, power, brilliance, beauty, or the perfect partner.
❯ They believe they can associate only with people of equal importance.
❯ They expect special favors and unquestioning compliance from others and take advantage of them to get what they want.
❯ They are unwilling and unable to recognize anyone else’s needs and feelings. - ❯ They believe they are envied.
TREATMENT
❯ Antisocial PD Cognitive behavioral therapy ; however, person may seek help only when ordered to do so by court because of their criminal behavior.
❯ Borderline PD Dialectical behavior and mentalizationbased therapies combining psychodynamic , cognitive behavioral , systemic , and ecological approaches, and art therapy . Group psychotherapy if symptoms are mild; coordinated care program for moderate-to-severe symptoms.
❯ Histrionic PD Supportive and solution-focused psychotherapy to enable emotion regulation; however, treatment is difficult as individual often exaggerates ability to function.
❯ Narcissistic PD Psychotherapy to help the person understand the cause of their emotions and regulate them.
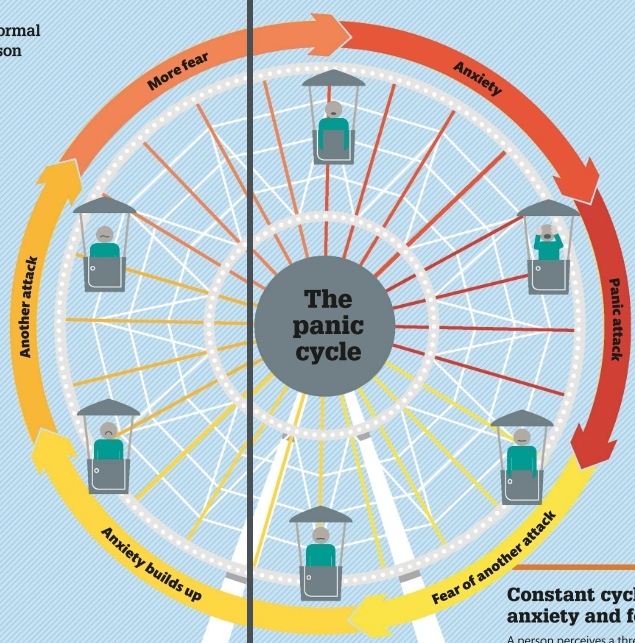
Cluster C: anxious/fearful
This group of personality disorders is characterized by worried, fearful thinking or behavior. A person with one of these disorders struggles with persistent and overwhelming feelings of fear and anxiety and may show patterns of behavior that most people would regard as antisocial and withdrawn. Cluster C includes dependent, avoidant, and OC (obsessive compulsive) PDs. A psychiatric assessment is needed to differentiate between dependent (below) and borderline PD , because the two share some symptoms.
- Dependent PD
- ❯ The person fears being on their own and having to fend for themselves.
❯ They constantly try to please and avoid disagreeing with people, because they are afraid of disapproval.
❯ They are oversensitive to criticism and pessimistic. - ❯ They lack self-confidence, suffer from self-doubt, belittle their abilities and assets, and may describe themselves as “stupid.”
❯ They display needy, passive, submissive, and clinging behavior, and may tolerate abuse.
❯ If a close relationship fails, they urgently seek another one. - ❯ They are often unable to start tasks for fear of failure.
- Avoidant PD
- ❯ The person fears criticism, disapproval, or rejection so strongly that they find it difficult to make connections with people.
❯ They are extremely cautious in creating friendships. - ❯ They are reluctant to share personal information or feelings, which can make it difficult to maintain the relationships they do have.
❯ They avoid any work activities that involve interpersonal contact.
❯ They stay away from social situations because they strongly believe they are inadequate and inferior. - ❯ They worry constantly about being “found out” and others rejecting, ridiculing, or shaming them.
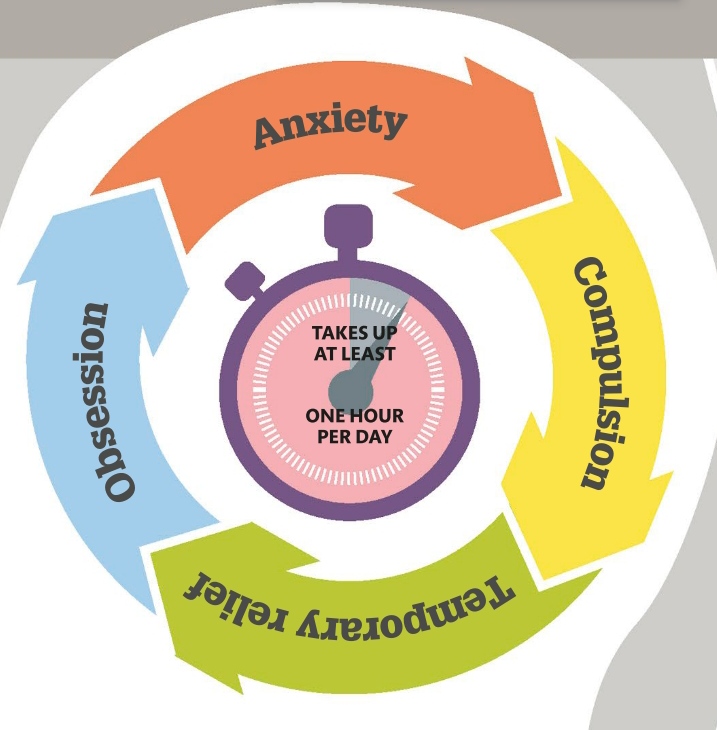
Obsessive compulsive PD
- ❯ The person is preoccupied with orderliness, perfectionism, and mental and interpersonal control.
- ❯ They are rigid and stubborn in pursuit of their principles.
❯ They are so devoted to work that they neglect friends and other activities, so they do not form or maintain meaningful social relationships.
❯ They are overconscientious and scrupulous and may miss work deadlines because they persistently aim for perfection. - ❯ They are inflexible on matters of morality or ethics.
- ❯ They are unable to discard worn-out or worthless objects even when they have no sentimental value.
10%
the estimated percentage of the global population affected by some form of personality disorder











")
")






")


")
")





")









")
")